Body weight continues to increase worldwide primarily because of the increase in body fat. This study analyzes the frequency of massive adiposity at autopsy determined by the ability of the heart to float in a container of 10% formaldehyde (because adipose tissue is lighter than myocardium) and compares certain findings in the patients with floating to those with nonfloating hearts. The hearts studied at necropsy during a 2-year period (2013 to 2014) at Baylor University Medical Center were carefully “cleaned” and weighed by the same person and tested as to their ability to float in a container of formaldehyde, an indication of severe cardiac adiposity. Of the 146 hearts studied, 76 (52%) floated in a container of formaldehyde and 70 (48%) did not. Comparison of the 76 patients with floating hearts with the 70 with nonfloating hearts showed significant differences in ages (62 ± 13 vs 58 ± 14 years). No significant differences between the 2 groups were found in gender, body mass index, frequency of systemic hypertension or diabetes mellitus, either acute or healed myocardial infarction, or whether death was due to a coronary or a noncoronary condition. A weak correlation was found between body mass index and heart weight in both men and women and in both floating and nonfloating hearts. The massive quantity of cardiac adipose tissue (floating heart) appears to have increased enormously in recent decades in the United States.
verweightness including obesity is now a worldwide problem. One commercial airline (Samoa Air) now bases ticket costs on body weight plus luggage. Although the fattest major US cities seem to vary each year, Houston, San Antonio, El Paso, and Dallas rank high in virtually every annual survey. Houston has more fast food outlets than any city in the United States. We studied the frequency of massive fatty deposits in the heart at necropsy during a 2-year period (2013 to 2014) in a single hospital located in Dallas and also compared various clinical variables in the floating versus nonfloating hearts studied during the same period.
Methods
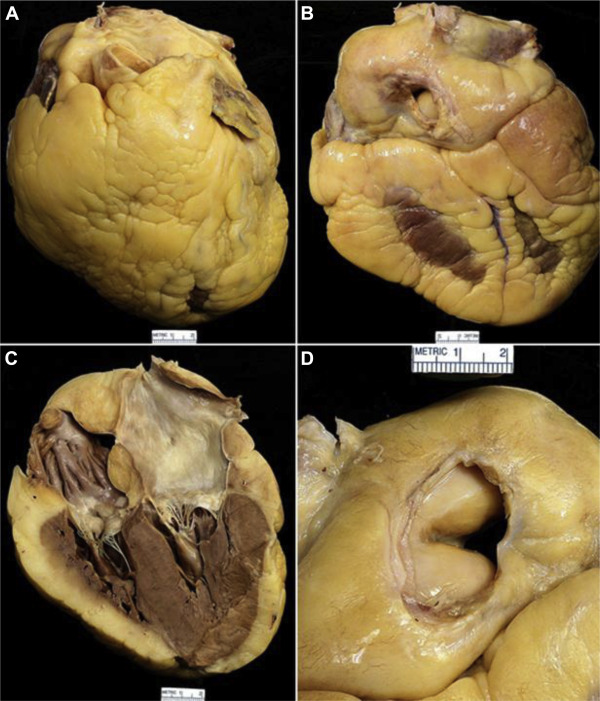
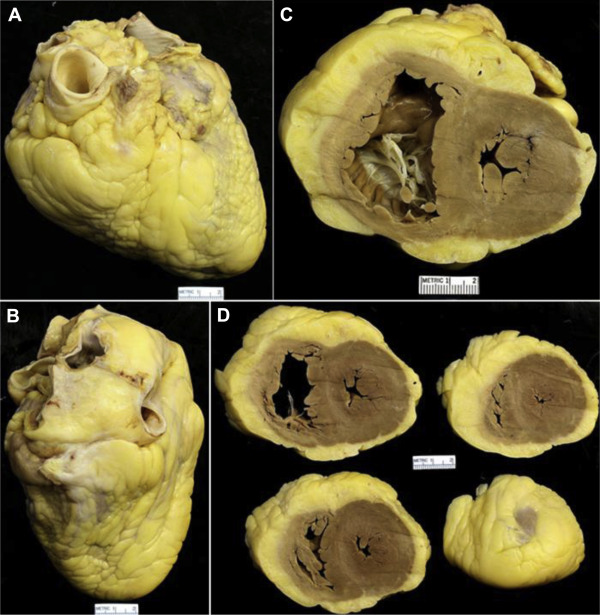
Because adipose tissue is lighter than cardiac muscle, hearts with enormous quantities of fat tend to float in containers of 10% formaldehyde and often in water.
During 2013 and 2014, Dr. Joseph M. Guileyardo, head of the autopsy service at Baylor University Medical Center, performed a total of 165 autopsies on adults. In 8, the autopsy permit did not allow examination of the heart; in 3 others, the autopsy was in patients who had previous cardiac transplantation. Of the remaining 154 autopsies in adults, WCR examined and described the hearts in 146 (95%). This study is limited to these 146 cases.
The hearts were “cleaned” of extraneous tissues, such as parietal pericardium, and then placed in a container of 10% fresh formaldehyde to determine if the heart floated to the surface after carefully removing any residual air from each chamber by compressing the heart several times when it was submerged. The heart was incised in various fashions depending on the perceived cardiac condition present (or absent) and weighed after gently “patting” all exposed surfaces by paper towels to remove extraneous water or formaldehyde. The scales used were accurate to 0.1 g (Ohaus Scott Pro Scale, Parsippany, New Jersey) or to 1.0 g (Acculab Vicon Digital Scale, Arvada, Colorado). All hearts were weighted by WCR.
The anterior surfaces of many of the 146 hearts were photographed, and, after opening, all hearts were photographed (by JMK). The clinical records were then obtained on each of the 146 patients through Baylor Health Care System’s electronic medical record (Allscripts Sunrise Enterprise, Chicago, Illinois).
Statistical analysis was done using STATA 14.0. The baseline characteristics of patients with floating and nonfloating hearts were compared using the chi-square or Fisher’s exact tests for proportions and t test/Wilcoxon’s rank-sum test for continuous variables where applicable. In addition, comparisons were conducted separately for men and women. Correlations among heart weight, age, and body mass index (BMI) were evaluated using Pearson’s correlation analysis. For correlation analyses, the data were rendered normal by removing any outliers.
Results
The major finding in this study was the high frequency of massive cardiac adiposity (as determined by whether the heart floated in a container of formaldehyde) at necropsy ( Figures 1 to 3 ). Of the 146 hearts, 76 (52%) contained such large quantities of adipose tissue that they floated and 70 (48%) did not float.
The second finding was comparison of various clinical and morphologic variables in the patients with floating versus nonfloating hearts ( Table 1 ). As shown in the accompanying table, age was the only variable that was significantly different between the 76 patients with floating hearts (62 ± 13 years) and the 70 patients with nonfloating hearts (58 ± 14 years). Women with floating hearts were older (62 ± 13 years) compared with those with nonfloating hearts (52 ± 15 years), whereas no difference in age was noted among men. Comparison of the patients with floating hearts versus nonfloating hearts showed no significant differences in gender, BMI, frequency of systemic hypertension or diabetes mellitus, heart weight, either acute or healed myocardial infarcts or both at necropsy, or whether death was due to coronary or noncoronary disease ( Table 1 ). The mean heart weights were larger in the men than in the women whether the heart floated or did not float.
| Variable | Total (N=146) | Float (n=76) | Nonfloat (n=70) | p Value |
|---|---|---|---|---|
| Age (years) (Mean±SD) | 60±13 | 62±13 | 58±14 | 0.03 |
| Range [median] | 23-90 [60] | 30-87 [62] | 23-90 [58] | |
| Men | ||||
| Mean±SD | 62±13 | 63±14 | 61±12 | 0.39 |
| Range [median] | 30-90 [63] | 30-87 [65] | 42-90 [59] | |
| 21-40 | 3/81 (4%) | 3/3 (100%) | 0/3 (0%) | |
| 41-60 | 35/81 (43%) | 12/35 (34%) | 23/35 (66%) | |
| 61-80 | 34/81 (42%) | 17/34 (50%) | 17/34 (50%) | |
| 81-100 | 9/81 (11%) | 5/9 (56%) | 4/9 (44%) | 0.11 |
| Women | ||||
| Mean±SD | 58±14 | 62±13 | 52±15 | 0.009 |
| Range [median] | 23-86 [58] | 37-86 [60] | 23-81 [52] | |
| 21-40 | 9/65 (14%) | 2/9 (22%) | 7/9 (78%) | |
| 41-60 | 31/65 (48%) | 20/31 (65%) | 11/31 (35%) | |
| 61-80 | 20/65 (31%) | 13/20 (65%) | 7/20 (35%) | |
| 81-100 | 5/65 (8%) | 4/5 (80%) | 1/5 (20%) | 0.08 |
| Sex | ||||
| Men | 81/146 (55%) | 37/81 (46%) | 44/81 (54%) | 0.09 |
| Women | 65/146 (45%) | 39/65 (60%) | 26/65 (40%) | |
| Body Mass Index (kg/m 2 ) (Mean±SD) | 31±9 | 32±8 | 30±9 | |
| Range [median] | 15-72 [29] | 18-55 [30] | 15-72 [29] | 0.19 |
| Men | ||||
| Mean±SD | 31±9 | 32±8 | 31±10 | |
| Range [median] | 16-72 [29] | 21-48 [30] | 16-72 [29] | 0.52 |
| ≤25 | 19/81 (23%) | 7/19 (37%) | 12/19 (63%) | |
| >25-30 | 26/81 (32%) | 12/26 (46%) | 14/26 (54%) | |
| >30 | 36/81 (44%) | 18/36 (50%) | 18/36 (50%) | 0.65 |
| Women | ||||
| Mean±SD | 31±9 | 32±8 | 28±7 | |
| Range [median] | 15-55 [30] | 18-54 [30] | 15-42 [30] | 0.11 |
| ≤25 | 21/65 (32%) | 10/21 (48%) | 11/21 (52%) | |
| >25-30 | 13/65 (20%) | 10/13 (77%) | 3/13 (23%) | |
| >30 | 31/65 (48%) | 19/31 (61%) | 12/31 (39%) | 0.23 |
| Coronary Artery Disease | 53 (36%) | 29/53 (55%) | 24/53 (45%) | 0.63 |
| Healed myocardial infarct | 29 (20%) | 12/29 (41%) | 17/29 (59%) | 0.20 |
| Acute myocardial infarct | 16 (11%) | 11/16 (69%) | 5/16 (31%) | 0.19 |
| Both | 3 (2%) | 2/3 (67%) | 1/3 (33%) | 1.00 |
| Neither | 13 (9%) | 8/13 (62%) | 5/13 (38%) | 0.57 |
| Diabetes Mellitus | 54 (37%) | 29/54 (54%) | 25/54 (46%) | 0.76 |
| Hypertension | 95 (65%) | 48/95 (51%) | 47/95 (49%) | 0.61 |
| Heart Weight (g) Mean±SD | 490±143 | 469±124 | 512±160 | 0.07 |
| Range [median] | 142-1070 [475] | 208-830 [455] | 142-1070 [488] | |
| Men | ||||
| Mean±SD | 548±135 | 519±108 | 572±151 | 0.08 |
| Range [median] | 335-1070 [515] | 335-720 [505] | 375-1070 [547.5] | |
| >400g | 72/81 (89%) | 32/72 (44%) | 40/72 (56%) | 0.53 |
| Women | ||||
| Mean±SD | 417±119 | 422±121 | 410±118 | 0.68 |
| Range [median] | 142-830 [410] | 208-830 [395] | 142-735 [410] | |
| >350g | 45/65 (69%) | 27/45 (60%) | 18/45 (40%) | 1.00 |
Figure 4 graphically shows the relation between BMI and heart weight in both floating and nonfloating hearts in both men and women. A weak positive correlation was found. Most hearts were of increased weight (>350 g in women and >400 g in men). Figure 5 graphically shows the relation of heart weight to age in both men and women and also the relation of the 2 variations to whether the heart floated. These relations were negative.



