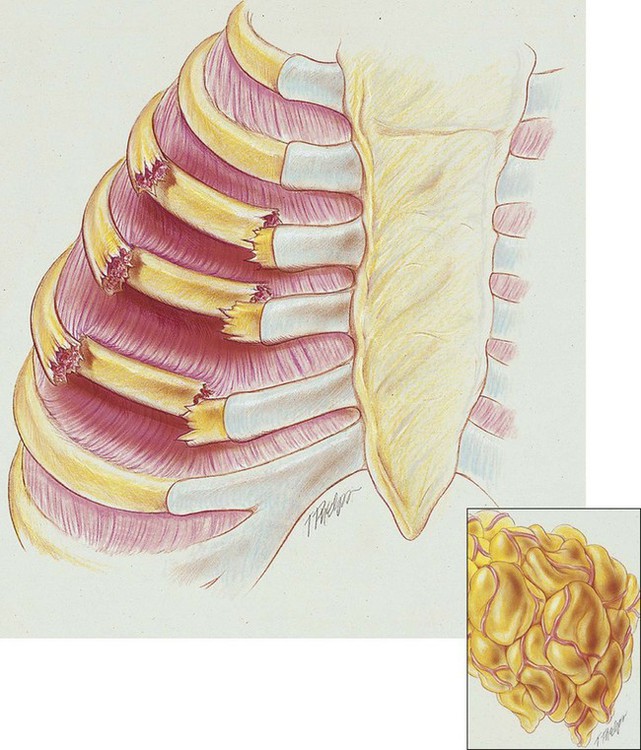
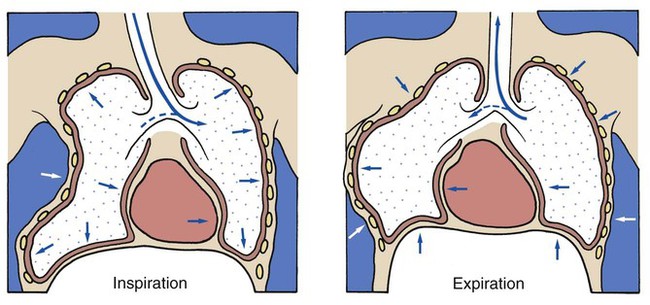
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with a flail chest. • Describe the causes of a flail chest. • List the cardiopulmonary clinical manifestations associated with a flail chest. • Describe the general management of a flail chest. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. A flail chest is the result of double fractures of at least three or more adjacent ribs, which causes the thoracic cage to become unstable—to flail (see Figure 21-1). The affected ribs cave in (flail) during inspiration as a result of the subatmospheric intrapleural pressure. This compresses and restricts the underlying lung area and promotes a number of pathologies, including atelectasis and lung collapse. In addition, the lung also may be contused under the fractured ribs. The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8) and Consolidation (see Figure 9-9)—the major anatomic alterations of the lungs associated with flail chest (see Figure 21-1). CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE Increased Respiratory Rate (Tachypnea) Paradoxic Movement of the Chest Wall When the lung on the affected side is compressed during inspiration, gas moves into the lung on the unaffected side. During expiration, however, air from the unaffected lung moves into the affected lung. The shunting of air from one lung to another is known as pendelluft (Figure 21-2). As a consequence of the pendelluft, the patient rebreathes dead-space gas and hypoventilates. In addition to the hypoventilation produced by the pendelluft, alveolar ventilation also may be decreased by the lung compression and atelectasis associated with the unstable chest wall. As a result of the pendelluft, lung compression, and atelectasis, the
Flail Chest
Anatomic Alterations of the Lungs
Etiology and Epidemiology
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Flail Chest
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Flail Chest
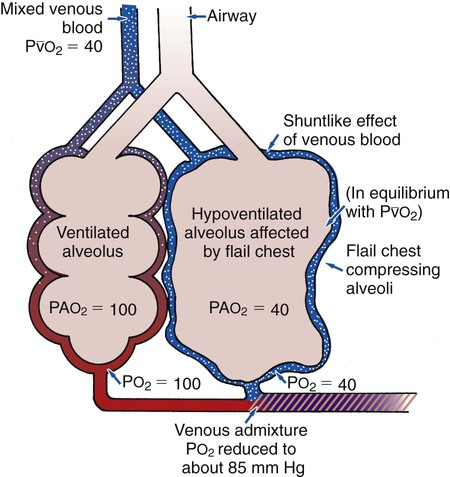
 ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 21-3). Because of the venous admixture, the patient’s Pao2 and Cao2 decrease. As this condition intensifies, the patient’s oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors, which in turn initiate an increased ventilatory rate.
ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 21-3). Because of the venous admixture, the patient’s Pao2 and Cao2 decrease. As this condition intensifies, the patient’s oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors, which in turn initiate an increased ventilatory rate.