Fetal and Enteric Carcinoma
Marie-Christine Aubry, M.D.
General Overview
In addition to mucinous and colloid carcinomas, “variants” of adenocarcinomas according to the WHO include fetal and enteric carcinomas. Fetal carcinomas overlap with pulmonary blastomas, which are classified as a subtype of sarcomatoid carcinoma and are biphasic tumors with a fetal adenocarcinoma component and a malignant-appearing immature stroma (see Chapter 85). Fetal adenocarcinomas lack the malignant stromal component.
Enteric adenocarcinoma is a term applied to primary lung tumors that histologically resemble colorectal carcinomas and can be confused with metastatic colorectal carcinoma to the lung.
Fetal Adenocarcinoma
Clinical
The clinical characteristics of fetal adenocarcinomas vary by their histologic subtype. Fetal adenocarcinomas that are low grade, with homogenous histologic findings, are typically seen in young to middleaged females with a modest or no smoking history. High-grade fetal adenocarcinomas present at a mean age in years in the low 60s and occur mostly in male smokers.
High-grade fetal adenocarcinomas account for <0.5% of adenocarcinomas of the lung.1 Low-grade fetal adenocarcinomas are rare tumors and are less common than the high-grade variant. It was initially described in 1984 as “well-differentiated adenocarcinoma simulating fetal tubules”2 and later in 1994 as “pulmonary endodermal tumor resembling fetal lung.”3
Microscopic Findings in Low-Grade Fetal Adenocarcinoma
Well-differentiated fetal adenocarcinoma is composed of glycogenrich glands and tubules that resemble fetal lung at 10 to 15 weeks of gestation.2,4 The tumor cells are cuboidal to columnar cells, with minimal atypia, and are arranged in complex structures and small rosettes, with apical cytoplasmic vacuoles (Fig. 77.1). Squamous morules are common. Areas of necrosis may occur but are less frequent than in high-grade tumors.
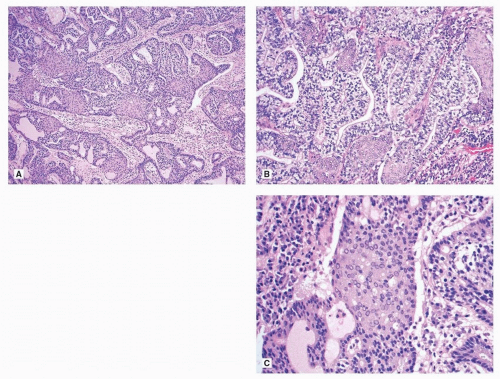 FIGURE 77.1 ▲ Fetal adenocarcinoma, low grade. A. The tumor is composed of glands that are often configured in a cribriform pattern. Several morules are present. The stroma is composed of benign spindle cells in a myxoid background. B. The glands are lined by columnar cells with a clear cytoplasm. The cell atypia is minimal. C. The morules are solid with polygonal cells containing eosinophilic cytoplasm. The main characteristic is the optically clear nuclei. |
The intervening stroma is scant and composed of benign spindled myofibroblastic cells. The presence of immature cellular stroma, with or without heterologous elements, warrants a designation of pulmonary blastoma (Chapter 85).4,5
Periodic acid-Schiff (PAS) staining demonstrates glycogen within the cytoplasm of the cells. Mucicarmine and PAS staining with diastase are negative.
Microscopic Finings in High-Grade Fetal Adenocarcinoma
High-grade fetal adenocarcinomas have, in addition to fetal lung-like areas, prominent nuclear atypia, a lack of morules, and a transition to conventional adenocarcinoma (Fig. 77.2). The term “blastomatoid variant of carcinosarcoma” is sometimes used for tumors with highgrade fetal lung-like epithelium and malignant spindled cell component (see Chapter 85).5
High-grade fetal adenocarcinomas show complex glandular, cribriform, and papillary structures, columnar cells with clear cytoplasm, supranuclear or subnuclear vacuoles, pseudostratified nuclei, and prominent nuclear atypia (Fig. 77.2). There are flat apical borders, absence of morules, and membranous or nuclear staining for β-catenin.1
The amount of tumor resembling fetal adenocarcinoma is quite variable. At least 5% of a given tumor must have areas typical of the entity according to published reports.1,5 However, the WHO requires 50%.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


