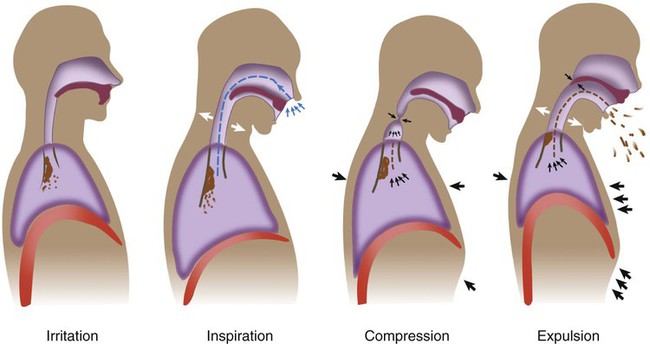
Cough is one of the most frequently reported symptoms in patients with pulmonary impairments. It is important to get a good history and physical examination to determine the cause and course of the patient’s cough.1 History should include sudden onset versus chronic; duration and type of cough—productive, nonproductive, or wheezy; whether the cough disturbs sleep and function; and what relieves or aggravates it. Diagnostic testing may include chest imaging, pulmonary function tests, bronchoscopy, and evaluation for gastroesophageal reflux (GER).2 GER is said to be the causative factor in up to 41% of adults with chronic cough.3 Frequent coughing or throat clearing may signal that the airways are irritated, that mucus is not clearing normally, or that the person is in an uncomfortable situation. This is something to be aware of, especially when treating patients with cystic fibrosis or asthma and patients with psychogenic issues. Depending on the reason for a cough, a variety of different approaches might be utilized. In most patients with primary pulmonary disease, the cough is related to the need for improved hydration and airway clearance. With patients who have psychogenic coughs, psychotherapy, biofeedback, and relaxation techniques have proven to be effective.4 Medications to suppress a cough are used rarely, primarily in the case of nonproductive, inflamed airways. Future directions are moving toward better medical management of cough reflex hypersensitivity through better diagnosis and medication.5 If the cough is productive, hydration and coughing are necessary to expel secretions to prevent pneumonia from occurring. Frequent coughing or throat clearing may indicate other problems besides airway clearance deficits. For example, a patient may have postnasal drip from a sinus infection or allergy. When the mucus drips down into the back of the throat, it can cause a reflex cough to clear it. Other causes include bronchogenic carcinoma, nervousness, and smoking. Many over-the-counter products are marketed to improve environmental air factors, but there has been conflicting evidence for their effectivess.6 In a pediatric patient with a cough, a foreign body or object inserted or inspired into the nose or airway should be ruled out. Gastroesophageal reflux must be evaluated in children and adults with symptoms of cough.7,8 GER is often overlooked in children. For example, if a child is beginning to prop-sit and pushes back to get out of that posture regularly, it may be because of GER irritation. This can delay developmental postures, so it is an important consideration for pediatric therapists. A persistent cough or throat clearing might be indicative of asthma or other pulmonary diseases, but it may also be a result of GER and irritation to the upper airway. It is important to ask questions related to the patient’s sleep. For example, does the person have heartburn or belching at least once a week after going to bed? Is there breathlessness at rest and nocturnal breathlessness? In a random group study in a large population of young adults, 4% were found to have GER. People with asthma and GER (9% of asthmatics had GER) had more nocturnal cough and morning phlegm with sleep-related symptoms.9 The authors concluded that there was a strong association between asthma and GER. Many patients with asthma find cough to be a more irritating, difficult symptom than wheezing and secretions. Yet cough is often not taken as seriously, even though it can be a life-interrupting symptom. Night cough can be a particularly difficult symptom in people with asthma and will make sleep difficult.10 Persistent cough has also been reported following pulmonary resection. The cause seems to be unclear, but some studies have focused on the population of patients who have had a lobectomy and mediastinal lymph node resection, some of whom also had GER. These were at increased risk for continued cough, which was found to persist up to a year later. Of this group, 90% saw improvement in their coughing with medication.11 If a patient demonstrates retained secretions on radiography, encourage hydration (drinking water), use airway clearance mobilization techniques, and carefully evaluate the cough. Instruct the patient in controlled coughing when mucus is felt in the throat or upper airways (see Chapter 21). If a cough is associated with eating, drinking, or taking medications, the patient’s swallowing mechanism should be examined and evaluated. A barium swallow (“cookie swallow”) is a fluoroscopic study in which the patient is given an opaque liquid, and a moving picture is observed to determine whether there is aspiration into the trachea. Populations commonly in need of evaluation of swallowing are patients with neurological disorders, such as those that occur with cerebrovascular accident (CVA), amyotrophic lateral sclerosis (ALS), cerebral palsy, Parkinson disease, and multiple sclerosis (MS). Patients who have tracheostomy tubes may experience difficulty in swallowing because the tube inhibits the normal movement of the larynx during swallowing. The use of a Passey-Muir valve has been found to be clinically effective in restoring a more normal swallow in patients with a tracheostomy. Older adults with chronic cough should be carefully observed and monitored, because the chronic cough may be a defense mechanism to prevent aspiration.12 This is especially true if there are comorbidities such as a previous stroke. This list is not exhaustive; any patient who chokes when you offer fluids or who reports to you that food or water “goes down the wrong way” should be referred for evaluation of the swallowing mechanism. Patients with chronic cough can also experience stress urinary incontinence (SUI).13 This is often not reported to the therapist or physician because the patient is embarrassed or considers this a problem of aging rather than a condition related to the chronic cough. Such patients often do not realize that physical therapy treatment is available for SUI. This knowledge deficit has been found in adolescents and teenagers with cystic fibrosis, as well as in adults with COPD. Asking patients with chronic cough about SUI should be a part of the routine examination and evaluation. Making a referral to a pelvic floor therapist can make a difference in their quality of life as SUI is managed. Four stages are involved in producing an effective cough.14 The first stage requires inspiring enough air to provide the volume necessary for a forceful cough. Generally, adequate inspiratory volumes for a cough are noted to be at least 60% of the predicted vital capacity for that individual. The second stage involves the closing of the glottis (vocal folds) to prepare for the abdominal and intercostal muscles to produce positive intrathoracic pressure distal to the glottis. The third stage is the active contraction of these muscles. The fourth and final stage involves opening of the glottis and the forceful expulsion of the air. The patient usually is able to cough three to six times per expiratory effort. A minimal threshold of FEV1 (forced expiratory volume in 1 second) of at least 60% of the patient’s actual vital capacity is a good indicator of adequate muscle strength necessary for effective expulsion (Figure 22-1). Bach and Saporito (1996)15 established a minimal peak cough flow rate (PCFR) of 160 L/min to effectively clear secretions and to predict successful decannulation for patients with neuromuscular conditions. The use of a simple peak flow meter can help assess the cough. Drops in peak flow have been correlated in children, patients with spinal cord injury, and older adults who have a decreased ability to cough. Assessing PCFR is a simple clinical test that can objectively measure the patient’s ability to provide the exhalation phase of the cough.16–18 During a cough, alveolar, pleural, and subglottal pressures may rise as much as 200 cm H2O.14,19,20 1. Do not disregard posture. Rather than simply asking the patient to cough from whatever position he or she happens to be in, ask instead, “What position do you like to be in when you feel the need to cough?” Then ask the patient to assume that posture, or assist the patient in assuming a posture as close to the preferred posture as possible. Pay close attention to the patient’s choice. A patient should spontaneously choose a posture that lends itself to trunk flexion, which is necessary for effective expulsion and airway protection. A red flag, or inappropriate choice, would be a preference for coughing while supine, which involves the opposite: trunk extension and poor mechanical alignment for airway protection. 2. Now the patient is ready to demonstrate coughing. Do not make the mistake of asking a patient to “show me a cough” or he or she may simply “show you” a cough. It may not be the way the patient coughs to clear secretions. Instead, continue to set the patient up for success by asking him or her, “Can you show me how you would cough if you had secretions in your chest and you felt the need to cough them out?” With these instructions, you are asking the patient to show you something functional rather than theoretical. Cough effectiveness can now be assessed (Box 22-1). Guidelines for objective evaluation with pulmonary function tests have been indicated previously. This section focuses on analyzing the movement patterns during all four stages of a cough. An effective cough should maximize the function of each individual stage. Thus in most patients (other than those with COPD or asthma), the clinician should see a deep inspiratory effort paired with trunk extension, a momentary hold, and then a strong cough or series of expiratory coughs on a single breath while the patient moves into trunk flexion. Box 22-1 Positioning and Instruction to Improve Cough Effectiveness Did the patient spontaneously inspire a deep breath before coughing, or did he or she cough regardless of the inspiration or expiration cycle? Did the patient spontaneously use trunk extension, an upward eye gaze, or the arms to augment the inspiratory effort? Did the patient take enough time to inspire fully before coughing? If the patient inspires adequately, he or she should be able to sustain two to six coughs per expiratory effort for a cascade effect. Neurologically impaired patients who have inadequate inspiratory efforts usually present with only one or two coughs per breath and generally produce a quieter cough.21 If the patient cannot cough on demand (such as a young child or patient with cognitive impairment), ask the caretaker whether he or she has observed and/or heard the patient’s inspiratory breath and hold before a cough. If so, how effective did the patient’s process seem?
Facilitating Airway Clearance with Coughing Techniques
Cough Associated with Eating or Drinking
Complications of Coughing
Stages of Cough
Cough Evaluation
Stage 1: Adequate Inspiration
Thoracic Key
Fastest Thoracic Insight Engine