end-diastolic pressure and volume for myocardial contractility. When myocardial injury or disease improves, myocardial contractility returns, left ventricular ejection increases, and pulsatile flow resumes. Because decreased preload reduces contractile function of the ventricle, status of myocardial preload should be taken into account when evaluating myocardial contractility during ECMO.
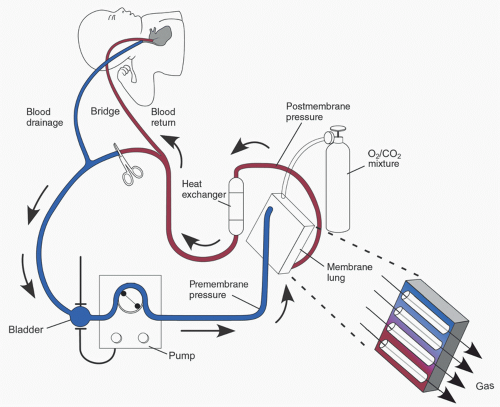 FIGURE 31.1. ECMO circuit in veno-arterial support mode. |
TABLE 31.1. Differences between veno-arterial and veno-venous ECMO modes | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
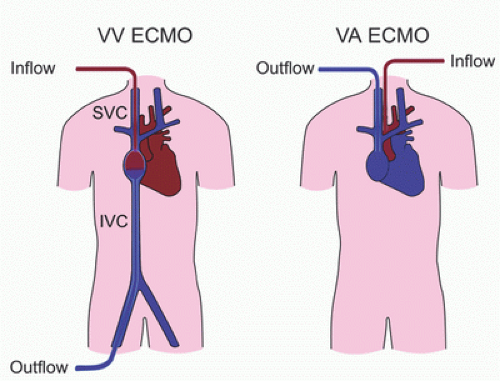 FIGURE 31.2. Veno-venous (VV) and veno-arterial (VA) ECMO. SVC, superior vena cava; IVC, inferior vena cava. |
 FIGURE 31.3. Pulmonary edema due to left atrial hypertension during veno-arterial ECMO. A: Pulmonary edema soon after ECMO cannulation; B: Resolution of pulmonary edema after balloon atrial septostomy. |
(28,29). Therefore, positioning the return limb of the venous cannula such that oxygenated blood from the ECMO circuit returning to the RA is directed toward the TV is crucial (Fig. 31.4). Recirculation of some oxygenated blood returned to the RA back into the venous drainage is common. However, recirculation of significant amounts of oxygenated blood results in reduced Sao2. Recirculation can be assessed by comparing the partial pressure of oxygen in the arterial (Pao2) and venous (Pvo2) limbs of the VV ECMO circuit. A Pvo2 <20% of the Pao2 is acceptable and does not impair the efficiency of VV ECMO (30). Decreased Sao2 during VV ECMO should prompt the evaluation of cannula position to ensure that oxygenated blood returned to the RA is directed toward the TV. Other causes of low Sao2 during VV ECMO include hypovolemia, RV dysfunction, increased pulmonary vascular resistance (PVR), and developing oxygenator failure. These issues should be promptly investigated and treated.
 FIGURE 31.4. Cannula position for veno-venous ECMO. SVC, superior vena cava; IVC, inferior vena cava; TV, tricuspid valve; RV, right ventricle; LV, left ventricle; Ao, aorta; PA, pulmonary artery. |
indicate that ECMO is being increasingly used to support neonates and children with postoperative cardiac failure following surgery for congenital heart disease (34).
TABLE 31.2. Indications for ECMO | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
made of reinforced material (e.g., Tygon S-95-E; Tygon, Saint-Gobain Corp., Courbevoie, France) to help withstand the shear stress imposed by the roller heads (51). Pump output is a function of pump speed (revolutions per minute; RPM), raceway tubing diameter, and degree of occlusion (43,50). To avoid direct suction to the venous catheter in roller pump ECMO circuits, a reservoir called the “bladder” is placed between the pump and the venous drainage tubing (52). Venous blood from the patient is drained passively by gravity into the bladder, limiting the direct application of negative suction pressure to the venous inflow and preventing injury to vascular structures and endothelium. A servo-control mechanism contained in the bladder regulates pump flow by decreasing pump speed when the bladder has reduced volume or is empty. This servo-control mechanism prevents cavitation and hemolysis from excessive negative pressure resulting from continued pump function when pump venous inflow is reduced or occluded and is thus an important safety feature for roller-pump ECMO circuits (53).
TABLE 31.3. Comparison of roller and centrifugal pumps | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
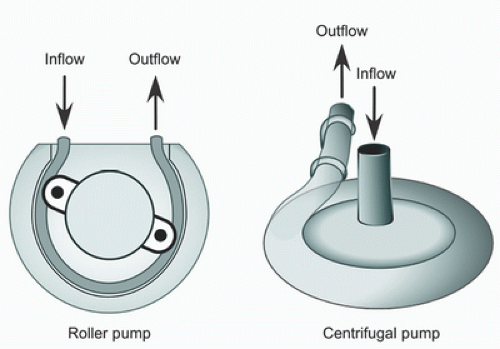 FIGURE 31.5. Schematic diagram of roller and centrifugal pumps. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


