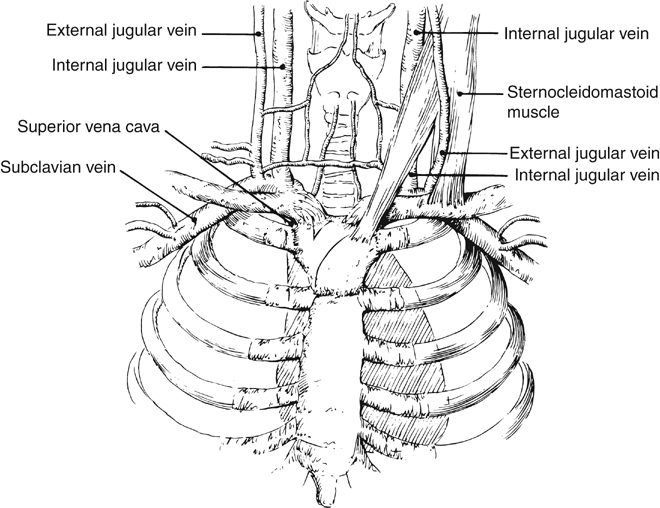
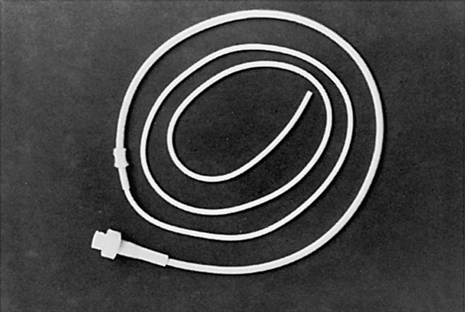
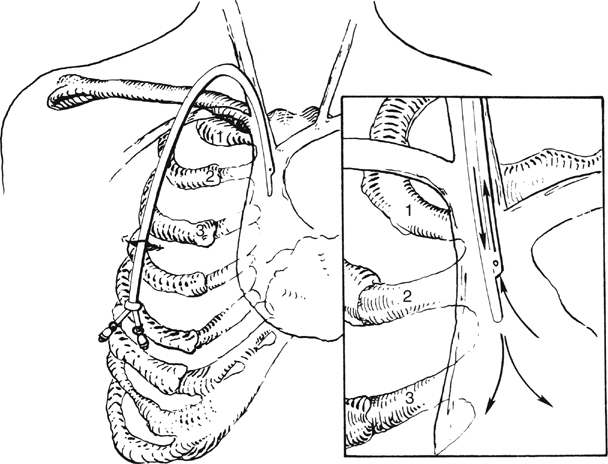
Juan Carlos Jimenez, Madhukar S. Patel and Samuel Eric Wilson Tunneled catheters were developed to facilitate long-term administration of IV therapy. Two commonly used tunneled devices are the Broviac and Hickman catheters. The Broviac catheter (Figure 1) was designed for prolonged infusion of TPN in children, and the Hickman catheter was developed to allow long-term central venous access in patients undergoing bone marrow transplantation. Both are now used for a variety of IV treatments, and they are also used in combination as a Hickman–Broviac double-lumen catheter. The catheters share many characteristics, including silicone elastic (Silastic) composition and a proximal cuff. The cuff anchors the catheter to surrounding soft tissues while also providing a mechanical barrier to infectious organisms. The main difference between these devices is catheter diameter. When using a Hickman–Broviac catheter, the smaller Broviac line is used for TPN or other forms of IV therapy. The larger Hickman line may serve as an additional line for IV therapy or as a source for blood withdrawal. When using either CVC, access may be achieved using the subclavian, internal jugular, or femoral veins. Portable ultrasound and fluoroscopy should be used routinely when placing these lines. The distal end is advanced to a location just above the right atrium, and the proximal end exits the lower anterior chest wall (Figure 2), anchored to the subcutaneous tissue by the cuff. Because of the silicone elastic composition, both catheters have low thrombogenicity but are susceptible to perforation or rupture. For this reason, guidewires should not be used to attempt clearance of obstructed catheters. Obstructed catheters should instead be irrigated using syringes no larger than 5 mL. Another recommended practice is to irrigate the lines with normal saline after any IV infusions to prevent occlusion or mixing of incompatible solutions. Hickman lines must be irrigated with heparinized saline after blood transfusions to prevent clot formation within the lumen. After placing the patient in the Trendelenburg position, the landmarks used for catheterization should be identified. An understanding of the anatomic relationships in this region is helpful (Figure 3). The subclavian vein arches over the first rib and passes posterior to the clavicle and anterior to the insertion of the scalenus anterior muscle. The vein is most easily accessed as it passes over the first rib. Both the lateral head of the sternocleidomastoid muscle and the division of the medial and middle thirds of the clavicle can serve as landmarks for this optimal site of catheterization.
External Methods of Angioaccess
Types of Central Venous Catheters
Acute-Care Devices
Tunneled Catheters
Techniques for Insertion
Internal Jugular Approach
Subclavian Vein Approach
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


External Methods of Angioaccess