(1)
Department of Neuroscience, University of Turin Ospedale Molinette, Turin, Italy
Abstract
The embryogenesis of the ECA can be summarized as follows. It is formed by the fusion of its proximal part with its distal segments. The proximal ECA develops from the ventral pharyngeal artery embryonal vessel arising from the primitive third aortic arch. The distal part develops from the hyoidostapedial artery, an embryological vessel arising from the future petrous segment of the ICA (see also Sects. 2.1 and 2.4.1.1).
The embryogenesis of the ECA can be summarized as follows. It is formed by the fusion of its proximal part with its distal segments. The proximal ECA develops from the ventral pharyngeal artery embryonal vessel arising from the primitive third aortic arch. The distal part develops from the hyoidostapedial artery, an embryological vessel arising from the future petrous segment of the ICA (see also Sects. 2.1 and 2.4.1.1).
The final external carotid artery arises from the common carotid bifurcation at the C4 vertebral level. A more proximal or distal origin can occur (see Sect. 2.1). Other rare variants are the origin of the ECA directly from the aortic arch and the so-called non–bifurcating cervical carotid artery (Morimoto et al. 1990; Uchino et al. 2011; Nakai et al. 2012). In this case, the typical carotid bifurcation is not recognizable with its typical trunk of ECA and ICA. The common carotid artery seems to continue directly in the trunk of ECA from which arise its branches. The ICA appears to be a continuation of the ECA. The interpretation of this anomaly is not completely clear (see also some aspects of the embryogenesis of ECA, ICA, and CCA in Sect. 2.1). According to some authors (Morimoto et al. 1990; Uchino et al. 2011; Nakai et al. 2012), we are dealing with a segmental agenesia of proximal ICA. The common carotid artery continues into the ECA which gives off its branches. The distal segment of the artery runs medially continuing into the distal ICA which in this case could arise from the occipital or ascending pharyngeal arteries. This theory could be confirmed by the fact that occasionally the origin of the occipital or pharyngeal arteries from the ICA can be visible on the angiogram (Figs. 2.12, 3.8a and 3.17d). Another possibility is a failure in the development of the proximal trunk of ECA (the primitive ventral pharyngeal artery) and persistence of the embryonic hyoid–stapedial system which supplies the vascular territory of the ECA.
The ECA lies in the carotid triangle, initially medial and anterior to the ICA, seldom lateral to it. More cranially, it runs anterolateral to the ICA. The internal jugular vein is located posterolaterally to the proximal ECA which more distally near the skull base is located laterally to the internal jugular vein (Figs. 2.1 and 2.2). During its course, the ECA gives off several branches and divides near the mandibular condyle within the parotid gland, into its terminal branches (the internal maxillary and the superficial temporal arteries, respectively, IMA and STA) (Figs. 3.1, 2.2, and 3.7).
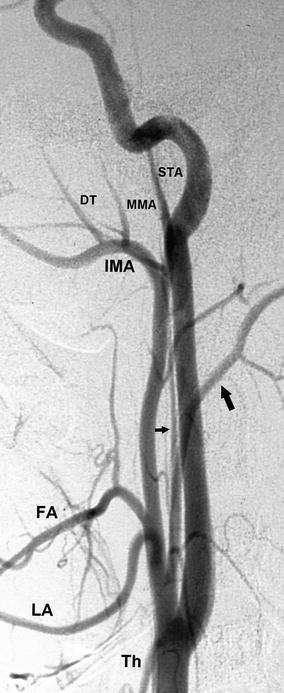
Fig. 3.1
Common carotid angiogram, lateral view, showing the anterior course of the external carotid artery related to the internal carotid artery. Some of the main branches are recognizable. Superior thyroid artery (Th), lingual artery (LA), facial artery (FA), occipital artery (large arrow), ascending pharyngeal artery (small arrow), internal maxillary artery (IMA), middle meningeal artery (MMA), middle deep temporal artery (DT), superficial temporal artery (STA)
3.1 Superior Thyroid Artery
The superior thyroid artery arises from the anterior wall of the ECA. It runs inferiorly and somewhat medially toward the thyroid gland. The superior thyroid artery gives off branches for the superior part of the thyroid gland and larynx. It anastomoses with the inferior thyroid artery, a branch of the thyrocervical trunk, arising from the subclavian artery (Figs. 3.1 and 2.2).
3.2 Lingual Artery
The lingual artery is the second branch of the ECA and arises from its anterior wall. It is not exceptional for the lingual artery to have a common trunk with the facial artery. It gives off branches for the sublingual and submandibular glands, the pharynx and mandibular mucosa, and the muscle of the floor of the mouth. Its terminal branch is the deep lingual artery, which supplies the muscle and lingual mucosa. On the angiogram, the lingual artery is easy to recognize, especially in the lateral view, because of its course, first upward, then downward, and finally upward again, forming a gentle curve that is superiorly concave. The ascending branches, which supply the tongue, are easily recognizable. Among the lingual artery’s branches, the dorsal lingual artery and the sublingual artery, which runs inferiorly to the deep lingual artery, are frequently identifiable. The sublingual artery anastomoses through its submental branch with the corresponding branch of the facial artery (Figs. 3.1, 3.2, and 3.3).


Fig. 3.2
External carotid artery angiogram, lateral view, showing the common trunk of origin (large arrow) of the lingual (small arrows) and facial arteries (arrows with dot)
Fig. 3.3
Selective angiographic study of the lingual artery. Branches for the tongue (arrows) arising from the main trunk and dorsal lingual artery (DL). Sublingual branches (arrow with angle)
3.3 Facial Artery
The facial artery is the third branch arising from the anterior wall of the ECA, sometimes with a unique trunk with the lingual artery. It runs forward, with an undulating course above the submandibular gland, to which it gives off some branches that are occasionally well developed; the facial artery then curves around the lower edge of the mandible, continuing anteriorly and superiorly and crossing the cheek before ending in the medial angle of the orbita as an “angular artery.” The latter anastomoses with branches of the ophthalmic artery, which can establish a collateral circulation when the ICA is occluded (Fig. 3.12). Along its course, the facial artery can anastomose with the transverse facial artery and with branches of the internal maxillary artery (IMA), especially with the infraorbital, buccal, and masseter arteries.
The facial artery gives off branches for the submandibular gland, masseter muscle, mandible, skin and muscle of the submental area, and the cheek, nose, and lip. From its initial segments arises the ascending palatine artery, which anastomoses with the pharyngeal branches of the ascending pharyngeal artery (APhA) and with the descending palatine artery of the IMA. The ascending palatine artery can be hypoplastic and replaced by branches of the APhA. The facial artery may be hypoplastic and represented only by the submental artery. In such cases, parts of its vascular territories becomes replaced by the lingual artery, transverse facial artery, and infraorbital artery (Djindjian and Merland 1978).
The initially descending and then the obliquely ascending course of the facial artery is easily discerned on the lateral angiogram. Among its branches, the ascending palatine artery, artery for the submandibular gland, and submental artery are the most frequently identifiable (Figs. 3.1, 3.2, and 3.4).
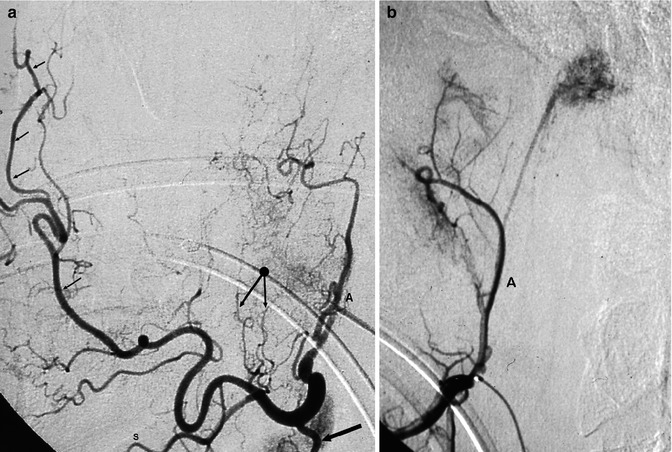
Fig. 3.4
(a) Selective angiographic study of the facial artery. Ascending palatine artery (A). Branches for the submandibular gland (arrow) and masseter muscle (arrow with dot). Submental artery (S), distal branches (small arrows) ending in the angular artery. (b) Different patient, selective study of the facial artery. Ascending palatine artery (A), from which arises a branch supplying a large vagal paraganglioma
3.4 Ascending Pharyngeal Artery
The APhA is a small vessel that arises from the posterior wall of the ECA, sometimes from the carotid bifurcation or from the proximal segment of the ICA. The APhA can also arise sharing a common trunk with the occipital artery. It runs upward adjacent to the ICA, posteriorly and medially to it (Figs. 3.5 and 3.6).
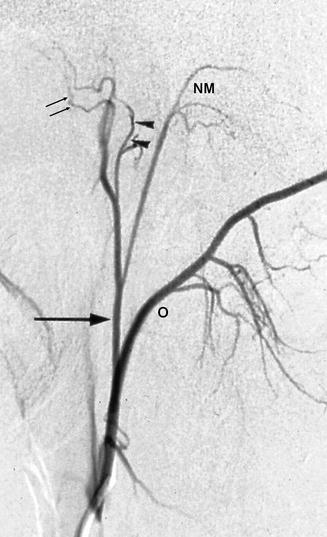

Fig. 3.5
Selective angiographic study, lateral view of the common trunk of the ascending pharyngeal and occipital arteries. Occipital artery (O), ascending pharyngeal artery (arrow) with its tympanic branches (arrowhead), superior pharyngeal branches (small arrows) and neuromeningeal trunk (NM)
Fig. 3.6
Common carotid angiogram, showing the close relationship of the ascending pharyngeal artery (arrow) with the internal carotid artery
The APhA gives off pharyngeal branches for the paramedian mucosa of the naso-oropharynx, which are divided into superior, middle, and inferior branches. The superior branch can anastomose with pharyngeal branches coming from the accessory meningeal artery and pterygovaginal artery, both branches of the IMA. The middle branches anastomose with the ascending palatine artery of the facial artery and, when present, with the mandibular artery, an embryological remnant arising from the ICA.
Other branches are the musculospinal arteries, which anastomose with branches of the vertebral artery at the C1–C2 level and also with branches of the occipital and ascending cervical arteries. Near the base of the skull, the APhA divides into its terminal branches, described in the following section:
1.
Superior pharyngeal branches.
2.
The inferior tympanic artery vascularizes the tympanic cavity and can anastomose with the other tympanic branches arising from the stylomastoid artery and IMA. There may also be an anastomosis with the caroticotympanic branch of the ICA, when present (Fig. 3.5).
3.
The neuromeningeal trunk can be subdivided into the hypoglossal and jugular branches (Lasjaunias et al. 2001; Djindjian and Merland 1978) (Fig. 3.5).
The hypoglossal branch enters the hypoglossal canal, running together with cranial nerve XII and with the anterior condylar vein. It gives off branches for the meninges of the adjacent posterior fossa and a descending branch that anastomoses with the ascending radiculomeningeal branch of the vertebral artery, contributing to form the so-called odontoid arch; see also Sect. 6.1.1. (Figs. 3.8c, 6.2b, c, 6.3, 6.9c, 13.3a, b, 15.19, 15.20, 3.29, and 3.30). The artery also gives off meningeal branches, which extend upward along the clivus (clival branches), anastomosing with the corresponding medial clival branches of the meningeal hypophyseal trunk (MHT) of the ICA (Figs. 3.28). Because of this anastomosis, the neurohypophysis can sometimes be visible on the lateral angiogram of the APhA (Djindjian and Merland 1978).
The jugular branch enters the posterior fossa through the jugular foramen, where it supplies cranial nerves IX, X, and XI (Lasjaunias et al. 1978a, 2001). It supplies the adjacent dura, anastomosing with the more lateral, descending clival branches of the MHT; it then runs further posteriorly to vascularize the dura of the cerebellar fossa and cerebellopontine angle.
The supply of cranial nerves IX, X, Xi, and XII is a very important aspect that should be taken into consideration in the endovascular treatment of lesions involving the APhA. Furthermore, the close relationship of the APhA with the ICA could explain the palsy of the nerves in many cases of dissection of the ICA (Bradac et al. 1990, 2000) (Fig. 3.6). The branches of the APhA may be involved in different pathological processes (Figs. 3.19, 3.21, 3.22, 3.23, 3.24, 13.3a, b, 13.4, 13.11, 13.17, 13.18, and 13.19).
3.5 Occipital Artery
The occipital artery takes its origin from the posterior wall of the ECA, frequently as a common trunk with the APhA (Figs. 3.5 and 3.8). The occipital artery can sometimes arise from the vertebral artery or ICA (Fig. 3.8). It runs posteriorly and slightly superiorly with an undulating course, in which three segments may be identified: the first ascending, the second horizontal, and the third ascending again. It gives off several musculocutaneous branches for the neck and posterior part of the head and meningeal branches, among which the following are the most important:
1.
The stylomastoid artery arises from the first segment and runs up to the stylomastoid foramen, accompanying the facial nerve supplying it. It anastomoses superiorly with the superior tympanic artery, arising from the petrosquamous artery branch of the middle meningeal artery. The stylomastoid artery also gives off branches for the tympanic cavity and adjacent area (posterior tympanic artery), where they anastomose with the other tympanic branches arising from the APhA and IMA. The stylomastoid artery can arise from the posterior auricular artery or directly from the trunk of the ECA. It is a fine branch, not always evident on the lateral ECA angiogram. It can be dilated and well recognizable when involved in the supply of pathological processes (Figs. 3.22, 3.24c, and 13.1).
2.
Of the muscular branches, two arise in the ascending segment. A third branch (the splenial artery) arises from the horizontal segment, has a descending course, and supplies the splenius muscle. The muscular branches can anastomose with corresponding branches of the vertebral artery at the C1–C2 level and with branches of the ascending cervical artery (Figs. 3.7, 3.8, and 15.20).

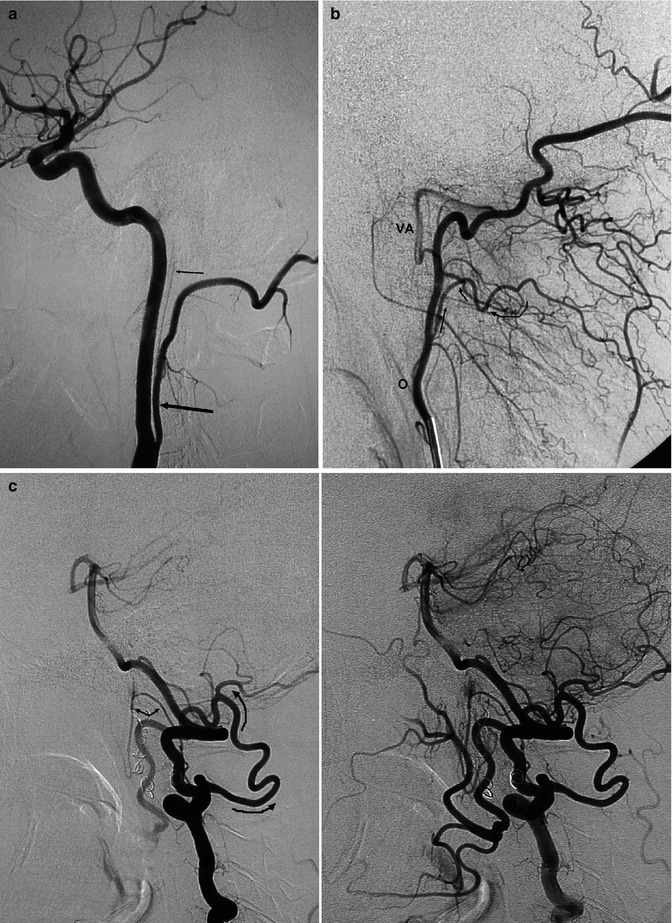
Fig. 3.7
Angiogram of the external carotid artery (lateral view). Occipital artery (O), with its muscular branches from the ascending segment and horizontal segment; splenial artery (S). Mastoid branch (M), posterior auricular artery (PA), superficial temporal artery (STA), internal maxillary artery (IMA)
Fig. 3.8
(a) Internal carotid angiogram, lateral view. Origin of occipital artery (arrow) from the internal carotid artery. The ascending pharyngeal artery (small arrow) arises as a common trunk from the occipital artery. (b) Selective angiogram of the occipital artery (O). There is an evident anastomosis (arrows) between the muscular branch of the ascendens segment of the occipital with the vertebral artery (VA). (c) Lateral vertebral angiogram (earlier and later phases) in a patient with proximal surgical ligature of the external carotid artery. Through anastomosis involving muscular branches of the VA and O (arrow) complete recanalization of the external carotid artery. Odontoid arch (arrow with angle) leading to a retrograde injection of the ascending pharyngeal artery
3.
The mastoid branch (Fig. 3.7) arises from the second segment, approximately near the origin of the splenial artery. It has an ascending course, enters the cranial cavity through the foramen of the emissary vein, and supplies the meninges of the cerebellopontine angle and cerebellar fossa. These branches are in hemodynamic balance with those arising from the neuromeningeal trunk of the APhA, with the petrosquamosal branch of the middle meningeal artery (MMA), and with the meningeal branches of the vertebral artery (Lasjaunias et al. 1978b). One of these branches can dominate and completely supply these territories.
3.6 Posterior Auricular Artery
This is a small branch arising near the terminal ECA (Fig. 3.7), sometimes as a common trunk with the occipital artery. It supplies the pinna of the ear, which is frequently evident as a blush in the capillary phase of the ECA angiogram.
3.7 Internal Maxillary Artery
The IMA is the larger of the terminal branches of the ECA. It originates behind the neck of the mandible, within the parotid gland. It runs obliquely forward and medially in the masticator space, along the border of the lateral pterygoid muscle and ends in the pterygopalatine fossa, where it divides into its terminal branches. It is always distinctive on the lateral and AP angiogram (Figs. 3.9, 3.10, and 3.11).
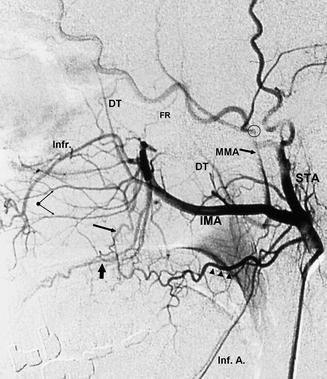
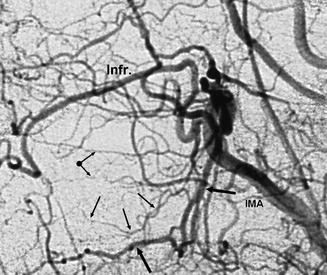
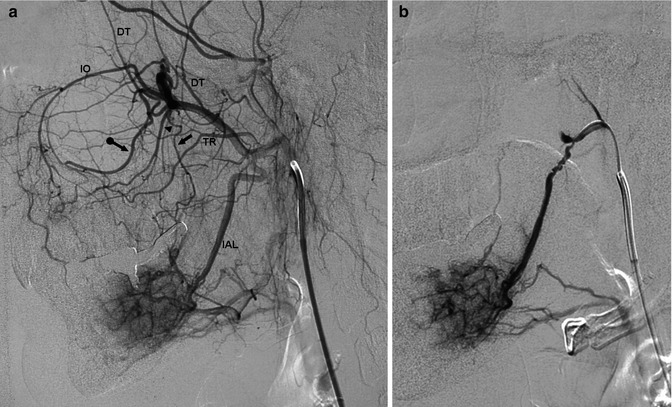
Fig. 3.9
Angiogram of the distal external carotid artery, lateral view. Transverse facial artery (arrowhead). Superficial temporal artery (STA), internal maxillary artery (IMA), middle meningeal artery (MMA). The circle shows where the MMA passes through the foramen spinosum. Middle and anterior deep temporal arteries (DT), inferior alveolar artery (Inf. A.), infraorbital artery (Infr.), posterior superior alveolar artery (arrow), descending palatine artery (large arrow), nasal branches of the sphenopalatine artery (arrows with dot), small foramen rotundum artery (FR)
Fig. 3.10
Angiogram of the distal external carotid artery, lateral view, detail. Internal maxillary artery (IMA), infraorbital artery (Infr.), posterior superior alveolar artery (small arrows), descending palatine artery (large arrow), nasal branches of the sphenopalatine artery (arrow with dot)
Fig. 3.11
(a) Angiogram of the distal external carotid artery performed to study a capillary-venous vascular malformation of the mandible. Dilated inferior alveolar artery (IAL) supplying the malformation. Transverse facial artery (TR), buccal artery (arrow), deep temporal arteries (DT), descending palatine artery (arrowhead), posterior superior alveolar artery (arrow with dot), infraorbital artery (IO). The distal branches of the sphenopalatine artery are evident as fine branches running between the infraorbital and posterior superior alveolar arteries (b) Selective catheterization of the IAL preceding embolization
3.7.1 Proximal Branches
Near its origin, the IMA gives off thin proximal branches for the mandibular joint, external auditory canal, and tympanic cavity (anterior tympanic artery). The latter can be involved in the vascularization of chemodectomas (Fig. 3.22).
3.7.1.1 Middle Meningeal Artery
The MMA is the first largest proximal branch of the IMA. It runs superiorly toward the base of the skull and passes through the foramen spinosum, becoming intracranial, running along the greater sphenoid wing, and forming a large convex curve anteriorly (lateral angiogram) and laterally (AP angiogram) (Figs. 3.9 and 3.13). It is the most important artery in the vascularization of the dura and gives off the following branches:
The MMA gives off arteries for the dura of the frontoparietal and temporo-occipital convexity.
It gives off branches for the frontobasal area, anastomosing with ethmoidal branches, arising from the ophthalmic artery.
A meningeal branch can enter the orbita through the superior orbital fissure or through the foramen of Hyrtl and anastomose with the lacrimal artery, a branch of the ophthalmic artery.
Branches for the middle cranial fossa, where they anastomose medially near the cavernous sinus with the meningeal branches supplying this area, arising from the inferolateral trunk (ILT), MHT, foramen rotundum artery, and accessory meningeal artery.
Close to the foramen spinosum arises the petrosquamous branch, which supplies the dura, covering the petrous bone, partially the tentorium, and extends largely in the posterior fossa; there, it anastomoses with the meningeal branches, supplying the dura of the posterior fossa arising from the APhA, occipital artery, and vertebral artery. The petrosquamous branch gives off a tympanic branch (superior tympanic artery), which runs in the petrous facial canal, where it anastomoses with the stylomastoid artery—a branch of the occipital or posterior auricular artery. These arteries can both supply the nerve, but there is commonly a predominance of the petrosquamous branch (Lasjaunias et al. 2001). Furthermore, the petrosquamous branch gives off branches for the tympanic cavity, where they anastomose with the anterior, posterior, and inferior tympanic arteries.
In the paramedian area of the convexity, the branches anastomose with those of the contralateral side. Furthermore, the branches form an arcade from anterior to posterior, situated at the insertion of the lateral wall of the superior sagittal sinus with the meninges of the vault. This arcade anastomoses anteriorly with the artery of the anterior falx, a branch of the anterior ethmoidal artery, and posteriorly with the falx cerebelli artery. The arteries of the falx itself arise from the arcade as descending branches.
Branches of the MMA are involved in the supply of extra- and intracranial tumors (Figs. 3.24, 3.25, and 3.26) and intracranial vascular malformations (Figs. 13.3, 13.8, 13.9, 13.10 and 13.11, 13.13, 13.15, and 13.20). Due to deviation in the embryological evolution, the MMA can be characterized by many variants (see Sect. 2.4.11).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


