Exercise Testing
Paolo T. Pianosi
David J. Driscoll
Accurate and reproducible measurement of work performance or exercise capacity can provide a wealth of information: (i) means to estimate disease severity; (ii) assess one aspect of quality of life; (iii) gauge the effects of intervention; (iv) offer prognostic information; (v) identify previously unrecognized disease in some instances. Changes in operative and perioperative management of congenital heart defects have led to improved survival of affected children, prompting development of adult congenital heart disease clinics. Over the past decade, a number of publications on exercise testing in adolescent and young adult survivors revealed several, novel, hitherto unanticipated observations highlighting the importance of clinical exercise testing in this population. This developed on a background of large-scale epidemiologic studies demonstrating the positive relationship between fitness—quantified by peak oxygen uptake ([V with dot above]O2)—and longevity. One need only consider the Barker hypothesis of early life origins of adult disease to understand the implications of findings obtained from clinical exercise testing in pediatric populations. That is to say, better fitness defined by peak oxygen [V with dot above]O2 is associated with longevity in healthy populations and evidence is accumulating that the same holds for patients with chronic disease.
Basic Exercise Physiology
Exercise involves utilization of energy and its transformation into mechanical work, that is, muscle contraction. From the mechanical perspective, there are two types of exercise: isotonic (dynamic) and isometric (static). Isometric exercise involves muscular contraction against a fixed resistance with little (if any) muscle shortening. Isotonic exercise implies alternate rhythmic contraction and relaxation of muscles against resistance, such as running or cycling. However, even though one typically presumes muscle contraction leads to shortening, this occurs only with concentric contraction. Eccentric contraction occurs as the load on the muscle increases until it finally reaches a point where the external force on the muscle is greater than the force that it can generate. In such a scenario the muscle is forced to lengthen due to the high external load even though it may be fully activated. Think of when one places a heavy object on a table below; the biceps must be taut, yet the elbow undergoes extension. The cross-bridge theory of muscle contraction readily describes concentric contractions but is incomplete in explaining eccentric contractions. Understanding this distinction can result in innovative ways to analyze regulatory mechanisms underlying the physiologic responses to dynamic exercise.
Clinical exercise testing is typically done using isotonic forms of exercise, wherein there is alternate rhythmic contraction and relaxation of muscles against resistance, virtually always concentric. From the energetics perspective, the chemical energy required to perform work can arise from aerobic or anaerobic sources. Oxygen ultimately is required for ATP synthesis through mitochondrial oxidative phosphorylation in light to moderate, so-called aerobic, exercise. In contrast, short sprints, isometric exercise, or heavy isotonic exercise can be accomplished without oxygen for brief periods. In anaerobic exercise, muscle energy is supported by the phosphocreatine (PCr)-ATP system followed by glycolysis, which has a much lower yield for ATP production and comes at the price of increasing lactic acid production. During incremental exercise, one can observe a level of work or intensity of exercise below which is allegedly accomplished aerobically, and above which is ostensibly done anaerobically, or at least anaerobic energy sources predominate. Many of these conclusions have been reached by gas exchange analysis or measurement of blood lactate levels. More recent results employing near-infrared spectroscopy (NIRS) paint a different picture—one demonstrating an early, continuous, but complementary role of anaerobic metabolism to the primacy of aerobic metabolism during exercise (1). Because energy is necessary to perform work and requires combustion of oxygen, there is a predictable relationship between aerobic work and oxygen consumption or uptake ([V with dot above]O2) as shown in Figure 11.1. This approximates 10 mL O2 per minute per watt in normal, healthy adults (2) but oxygen cost of work (mechanical efficiency) tends to be higher in children and is somewhat age-dependent (3). Because work equals force multiplied by distance, the unit for work is the newton-meter, or joule (J). There is a constant relationship between energy and work as described by the relationship one kilocalorie (kcal) being equal to 4.1868 joules (J). Power is work performed per unit time, expressed as joules/second, but commonly referred to as watt (W) (1 W = 1 J/s). Older nomenclature used the kilopond-meter (kpm), where one kilopond is the force acting on a 1 kg mass at the normal G-force (on earth), such that 1 W = 6.12 kpm/min.
If one excludes so-called tests of anaerobic capacity such as Wingate, exercise test strategies have evolved over the past
century from classical steady-state procedures—incremental or otherwise—to non–steady-state procedures. The latter have largely supplanted the former, and increments can be discrete (e.g., 1 to 2 minutes each) or continuous, also known as ramp protocols. The Bruce treadmill protocol likely achieves steady-state conditions in light to moderate exercise by virtue of its 3-minute stages. The difference between steady state and non–steady-state exercise can best be understood by considering energy utilization at onset of exercise. If one were to immediately change from walking to running on a treadmill, or unloaded pedaling to 50 W on a cycle ergometer, work rises in an instant but [V with dot above]O2 does not rise nearly so quickly. This step-up in power requires adjustments to ventilation and cardiac output in order to meet the energy requirement to perform the additional work. Until the cardiopulmonary system adapts to this increment, the exercising muscles utilize anaerobic energy sources such as ATP and PCr, replenished by rate-limiting glycolytic pathways. In doing so, the exercising muscles incur an O2 debt which is simply the area under the curve shown in Figure 11.2. Once the cardiopulmonary system has made the necessary transition in terms of ventilation and cardiac output, such that energy required to perform the additional work can be provided aerobically, exercise is considered steady state. The time course of the rise to steady state is described by a time constant (τ), and mathematically it can be shown that steady state is achieved over a time equal to approximately five to six time constants. The term exercise “kinetics” has been coined to describe this transition process. Time constants for HR and [V with dot above]O2, but not for cardiac output, have been reported in children (4) and are shorter (smaller) compared with adults (5). The distinction becomes an important consideration should one attempt to apply certain physiologic principles, such as solving the Fick equation, to non–steady-state exercise measurements. In general, measurements such as cardiac output that employ solving the Fick equation, or measurement of physiologic dead space by the Bohr equation, should be based on measurements done during steady-state exercise. That does not necessarily mean that non–steady-state measures of such parameters are invalid, but simply that they should be interpreted with caution. It has been amply demonstrated that many measurements made during non–steady-state, progressive exercise provide results or values very similar to those made during conventional, steady-state, tests. This is one reason, other than practicality, that non–steady-state, incremental or ramp exercise protocols largely have replaced the classical steady-state methods.
century from classical steady-state procedures—incremental or otherwise—to non–steady-state procedures. The latter have largely supplanted the former, and increments can be discrete (e.g., 1 to 2 minutes each) or continuous, also known as ramp protocols. The Bruce treadmill protocol likely achieves steady-state conditions in light to moderate exercise by virtue of its 3-minute stages. The difference between steady state and non–steady-state exercise can best be understood by considering energy utilization at onset of exercise. If one were to immediately change from walking to running on a treadmill, or unloaded pedaling to 50 W on a cycle ergometer, work rises in an instant but [V with dot above]O2 does not rise nearly so quickly. This step-up in power requires adjustments to ventilation and cardiac output in order to meet the energy requirement to perform the additional work. Until the cardiopulmonary system adapts to this increment, the exercising muscles utilize anaerobic energy sources such as ATP and PCr, replenished by rate-limiting glycolytic pathways. In doing so, the exercising muscles incur an O2 debt which is simply the area under the curve shown in Figure 11.2. Once the cardiopulmonary system has made the necessary transition in terms of ventilation and cardiac output, such that energy required to perform the additional work can be provided aerobically, exercise is considered steady state. The time course of the rise to steady state is described by a time constant (τ), and mathematically it can be shown that steady state is achieved over a time equal to approximately five to six time constants. The term exercise “kinetics” has been coined to describe this transition process. Time constants for HR and [V with dot above]O2, but not for cardiac output, have been reported in children (4) and are shorter (smaller) compared with adults (5). The distinction becomes an important consideration should one attempt to apply certain physiologic principles, such as solving the Fick equation, to non–steady-state exercise measurements. In general, measurements such as cardiac output that employ solving the Fick equation, or measurement of physiologic dead space by the Bohr equation, should be based on measurements done during steady-state exercise. That does not necessarily mean that non–steady-state measures of such parameters are invalid, but simply that they should be interpreted with caution. It has been amply demonstrated that many measurements made during non–steady-state, progressive exercise provide results or values very similar to those made during conventional, steady-state, tests. This is one reason, other than practicality, that non–steady-state, incremental or ramp exercise protocols largely have replaced the classical steady-state methods.
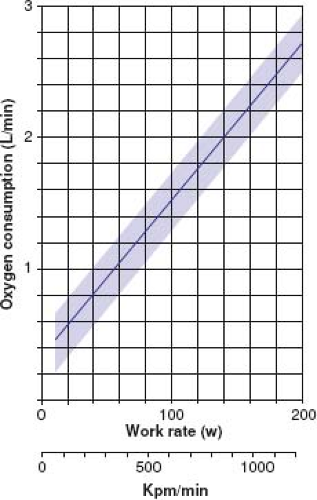 Figure 11.1 Diagrammatic illustration of the relationship between oxygen consumption and workload. (From Godfrey S. Exercise Testing in Children. London: WB Saunders Co. Ltd.; 1974.) |
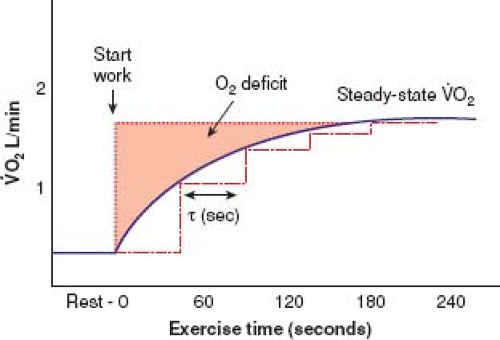 Figure 11.2 Schematic plot showing rest-work transition, plotting oxygen uptake versus time, in order to illustrate two concepts (i) oxygen deficit, that is, [V with dot above]O2 that would be required if all metabolic requirements to perform work were met instantaneously by aerobic mechanisms; and time constant (τ, seconds) which is the time required to reach 50% of the plateau value. As a rule, the plateau is reached in the equivalent time of five to six time constants. |
Exercise requires a complex and intricate interaction of multiple organ systems, and abnormalities in any of these organ systems will affect and potentially limit performance. The four principal systems involved in transferring oxygen from the atmosphere to the myocyte mitochondria—lungs, heart, blood, and muscle—are intimately linked in series and overall transport and utilization of oxygen depends on all components functioning optimally and in concert. Convection of oxygen from the atmosphere to exercising muscle will occur down a diffusion gradient starting with (a) its uptake in the lungs to saturate mixed venous blood; then (b) having a strong pump with an effective regulator that delivers enough O2 to the working tissues (including the diagphram) while limiting flow to “unnecessary” tissues; (c) having adequate and properly functioning hemoglobin such that uploading and downloading of adequate volume of O2 proceeds readily along its concentration (partial pressure) gradient; and ultimately (d) a high efficiency furnace (i.e., muscle capillaries and mitochondria) that rapidly downloads and utilizes O2 for fuel oxidation to produce adequate ATP to perform the task. When any one of these organ systems reaches maximal functional capacity, further exercise will be limited. An exercise test has the potential to reveal the limiting organ system, rather than provide a specific diagnosis in a patient presenting with exercise intolerance, by addressing the more fundamental question: whether oxygen supply (pulmonary/cardiovascular/blood transport), oxygen utilization (substrate availability, enzyme function) independent of oxygen supply, or converting chemical into mechanical energy (muscle efficiency) impose the limiting factor.
Exercise Testing Methods
Ergometry
Treadmill and stationary cycles are the two most frequently used ergometers for clinical exercise testing. Neither is inherently superior to the other; each has advantages and disadvantages. Most people can walk reasonably efficiently, but not everyone can cycle efficiently, particularly younger children. The relative merits and drawbacks of each modality are summarized in Table 11.1.
TABLE 11.1 Pros and Cons of Treadmill Versus Cycle Ergometry | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
The two general types of cycle ergometers are the mechanically braked and electronically braked. With a mechanically braked cycle ergometer, power varies with pedaling frequency; whereas with an electronically braked cycle ergometer, moderate changes in pedaling frequency do not affect power substantially. Thus, for younger or untrained subjects, who may have difficulty maintaining a steady pedaling frequency, electronically braked cycles are preferable. Mechanically braked cycle ergometers should be reserved for testing subjects who are cooperative, exercise regularly, and even then, steady cadence should be ensured by use of a metronome. The less frequently used arm-crank ergometer is useful for subjects who are unable to walk or cycle or for whom physiologic measurement of upper extremity function is of interest; for example, patients with spastic diplegia, leg weakness, or some patients with pulmonary disease in whom use of pectoral girdle musculature is a requirement not only for exercise but for breathing as well.
Exercise Protocols
There is no “best” exercise protocol. Examiners should select a protocol that best allows measurement of the responses to exercise that are of particular interest. Ideally, protocols should be standardized and data obtained for a “normal” population in the laboratory in which the clinical exercise testing is done. Power increments should not be excessive lest subjects stop exercise before a maximum effort has been achieved. Power increments that are too small result in unnecessarily long tests, which can be a challenge in a child who has a short attention span.
The Bruce protocol is arguably the most commonly employed treadmill protocol. For children and subjects incapable of much exercise, a modified Bruce protocol can be used in which the initial two steps use a belt speed of 1.7 mph and an incline of 0% and 5%, respectively (6). For cycle testing, step increments of 1-minute duration each (so-called Godfrey protocol (7)) or ramp protocols are becoming the norm. The ramp protocol uses a constantly increasing workload where the increment, regardless of magnitude, occurs as a gradual and continuous procedure instead of a step each minute. Regardless, exercise protocols should be designed such that the duration of the exercise test is 8 to 12 minutes. Obviously, a ramp protocol is not suited for assessing physiologic functions that require steady-state exercise. A good compromise is the standard incremental cycle ergometer protocol with increments in work every 1 or 2 minutes. The size of the increments should be tailored to the anticipated maximum capacity for optimal test duration as defined above, and yields enough data points to plot and analyze physiologic parameters with confidence.
Maximal Aerobic Power
Many different indices can be used to describe fitness or maximal exercise capacity. The amount of work a person can perform could be used to define exercise capacity but maximum aerobic power or maximum oxygen uptake ([V with dot above]O2max) achieved during exercise is probably the best. [V with dot above]O2max is defined by a plateau in [V with dot above]O2 that occurs despite continued exercise, proof that work can be performed using anaerobic energy production, but the amount that can be performed anaerobically is limited. This concept evolved using discontinuous, quasi–steady-state, exercise protocols nearly a century ago. A plot of [V with dot above]O2 versus work will reach an asymptotic [V with dot above]O2 if and only if the subject is able and willing to continue exercise, making it crucial to ensure a subject’s effort is maximal in order to properly determine [V with dot above]O2max. That said, determination of when such a plateau is achieved is somewhat arbitrary, and will vary with the sampling interval chosen—a selectable feature in all modern, breath-by-breath, metabolic carts (8). It is difficult to motivate untrained subjects or most children to exercise to that asymptotic
[V with dot above]O2, such that a plateau is seldom observed in children. For these reasons, the concept of [V with dot above]O2max has given way to the more practical “[V with dot above]O2peak” which will be used throughout this chapter. The terms [V with dot above]O2peak or peak work capacity have been coined to refer to a symptom- or fatigue-limited clinical exercise test, also known as voluntary exhaustion. Practically speaking, there is little difference between [V with dot above]O2peak and [V with dot above]O2max (9,10). In a maximal exercise test to voluntary exhaustion, most healthy subjects cease exercise because of leg discomfort or fatigue, though some will complain of dyspnea, as the reason(s) for being unable to continue. This presumably reflects leg muscle fatigue, where O2 demand exceeds O2 supply to (or utilization by) muscle.
Maximum cardiac output is correlated closely with maximum oxygen uptake (11). Oxygen supply to the exercising muscle is determined by oxygen carrying capacity (a function of hemoglobin) and rate of transport from the atmosphere to its destination, that is, cardiac output. This can be expressed mathematically as the product of cardiac output and oxygen content of the blood, that is, total oxygen transport capacity ([Q with dot above]O2). This has led to the conclusion that [Q with dot above]O2 is the factor limiting [V with dot above]O2max, although this concept continues to be the subject of debate among exercise physiologists. The opposing view is that muscle oxidative capacity is the true limit of maximum aerobic power based on strong correlations between either mitochondrial mass or capillary density in muscle (reviewed in ref. 12). If one subscribes to the convection hypothesis, it follows that reductions in cardiac output (or hemoglobin level) will lower [V with dot above]O2peak; conversely, experimentally increasing [Q with dot above]O2 (e.g., blood doping) will raise [V with dot above]O2peak. Exercising larger (vs. smaller) muscle groups or more (vs. fewer) muscle groups will result in higher [V with dot above]O2peak (12,13). It is for this reason that higher [V with dot above]O2peak can be achieved by treadmill than by cycle exercise. The larger exercising muscle mass is an important determinant of many exercise parameters, for example, greater muscle mass involved in exercise also dictates the relative contribution of stroke volume and heart rate in determining cardiac output during exercise. Indeed, lean leg volume or muscle cross-sectional area is perhaps the single best predictor of [V with dot above]O2peak (see below).
There are two important caveats to any conclusion or statement about [V with dot above]O2peak in children: one pertains to longitudinal versus cross-sectional study data and the other concerns the method of scaling or normalization of the data (as noted above). Investigators have searched for the best method of indexing [V with dot above]O2 and considerable controversy persists as to the best method, if one, indeed, exists. Based on the dimensionality theory, an exponent of body length was proposed by Astrand and Rodahl (14) who suggested using height raised to the power 2.9. Body weight (mass) expressed simply in kilograms has been criticized as a method for explaining growth-related changes because it led to spurious correlations, misinterpretation of data, and erroneous conclusions. Instead, exponents for weight ranging from 0.7 to 1.0 have been reported (15,16). This is particularly relevant given the current obesity epidemic. In the final analysis, the most commonly accepted and simplest method of indexing [V with dot above]O2 in clinical exercise testing is to use body weight (kilograms), but with recognition of the limitations of this approach. Said limitations become particularly relevant to compilation of normal reference standards which are inevitably derived from large cross-sectional sampling of a pediatric population, usually without regard to stage of physical development and pubertal maturation. Longitudinal studies have clearly shown that there are differences in the change of [V with dot above]O2peak over the age span 8 to 16 years. There are different individual trajectories for [V with dot above]O2peak during these growth years, which depend not only on age, sex, height, and weight; but also on trained versus untrained state (17,18). In essence, the so-called “normal range” is merely a composite of individual, single time-point, data. Thus, if one studies the same individual repeatedly over his/her growth years, which is probably more meaningful in the clinical arena, one must bear in
mind the pitfalls of applying normal population reference standards to an individual patient.
mind the pitfalls of applying normal population reference standards to an individual patient.
Because body mass, or better still, lean leg mass, increases considerably during the period of growth and maturation, [V with dot above]O2peak rises considerably when expressed in absolute terms (L/min), particularly in postpubertal males (Fig. 11.3A). There ought to be no difference between boys and girls in achievable values for [V with dot above]O2peak, at least not before puberty, if [V with dot above]O2peak were related to lean body mass. On the other hand, [V with dot above]O2peak normalized for weight (mL/kg/min) remains relatively constant in boys between ages 6 and 18 years; whereas in girls [V with dot above]O2peak remains relatively constant between the ages of 6 and 13 years, but levels off or even declines slightly after puberty in girls (Fig. 11.3B). This decline in girls probably represents the effect of increased body fat (or decreased lean body mass), perhaps coupled with the recently demonstrated trend in decreasing levels of daily physical activity in adolescent girls. Thus, in adolescence it is fair to say that boys have a higher [V with dot above]O2peak than girls, whether expressed in absolute or relative terms, but apart from this generalization the picture remains unclear. Prior to that age, [V with dot above]O2peak of boys and girls differs little although even this conclusion depends on the center, exercise protocol, and methods. There appear to be minor racial differences in [V with dot above]O2peak, at least in North American studies. Several small studies have shown lower [V with dot above]O2peak in African-American children compared with Caucasian children. African-American children have slightly smaller lung volumes than Caucasian children of similar standing height, and this alters ventilatory strategy during exercise slightly, but ventilation is not thought to limit exercise in health. One study concluded that slightly lower hemoglobin values and levels of habitual activity in African-American children accounted for part of the lower [V with dot above]O2peak observed (19).
Ventilatory Anaerobic Threshold
Considerable attention has focused on the so-called anaerobic threshold as a surrogate measure of maximal aerobic power. Theoretically, it might allow assessment of exercise capacity using a submaximal exercise study, a potential advantage in children who have difficulty achieving a true [V with dot above]O2peak. The term anaerobic threshold has given way to the term ventilatory threshold in recent years, in recognition of the fact that this time point during incremental exercise does not reflect the “onset” of anaerobic metabolism as was once hypothesized. The ventilatory (anaerobic) threshold (VT or VAT) is defined as the [V with dot above]O2 associated with a disproportionate increase in minute ventilation ([V with dot above]E) relative to [V with dot above]O2, signaled by a rise in percent mixed expired O2. There frequently is a disproportionate rise in lactate production at this point as well; hence the term anaerobic threshold (see Fig. 11.11) but an increased lactate is not necessary for the disproportionate rise in [V with dot above]E to occur (20). Breath-by-breath measurement of ventilatory indices and brief incremental workloads are preferable for determining the ventilatory (anaerobic) threshold. There are several methods of identifying this point, but the V-slope method is the most common and likely the most reliable in pediatrics (21). This point must also be distinguished from the second inflection or respiratory compensation point. At this juncture during incremental exercise, [V with dot above]E increases out of proportion to [V with dot above]CO2, such that [V with dot above]E/[V with dot above]CO2 also begins to rise, and end-tidal CO2 partial pressure begins to fall. This change is attributed to the H+-mediated drive to breathe created by blood lactic acid accumulation which has outstripped buffering capacity. Reybrouck et al. (22) reported an inability to detect a VAT in 10% of children. VAT was lower for girls than for boys. In normal boys, they found a gradual decrease in VAT between ages 8 and 16 years. When expressed as a percentage of [V with dot above]O2peak, VAT declined from approximately 65% in 8-year-old boys to approximately 55% in 16-year-old boys. It decreased from 62% in 8-year-old girls to approximately 55% in 16-year-old girls, similar to adult values. Apropos the earlier discussion pertaining to the concept of a “threshold” during an incremental exercise test, more recent NIRS indeed demonstrated (i) a strong correlation between lactate (ventilatory) threshold during incremental cycle exercise and exaggerated reduction in muscle oxygenation measured by NIRS and (ii) muscle deoxygenation trends recorded during short-duration, high-intensity exercise such as the Wingate test, indicate that there is substantial aerobic metabolism during such exercise (23).
Fitness
Improved fitness occurs with repetitive exercise—the “training effect.” From a strict physiologic standpoint, improved fitness implies an increase in [V with dot above]O2peak. Many studies in adults have demonstrated increases in [V with dot above]O2peak as a result of a conditioning or fitness program. In children, it has been more difficult to demonstrate this effect, probably because “normal” children simply are more fit than “normal” adults to begin with; hence, it is more difficult to demonstrate a change in fitness in normal children. However, a recent longitudinal study in athletic children
demonstrated that the type of physical activity did indeed affect the change in [V with dot above]O2peak during childhood (17). The importance of this observation may become more relevant in this era of increasing childhood obesity and decreasing fitness levels in today’s youth.
demonstrated that the type of physical activity did indeed affect the change in [V with dot above]O2peak during childhood (17). The importance of this observation may become more relevant in this era of increasing childhood obesity and decreasing fitness levels in today’s youth.
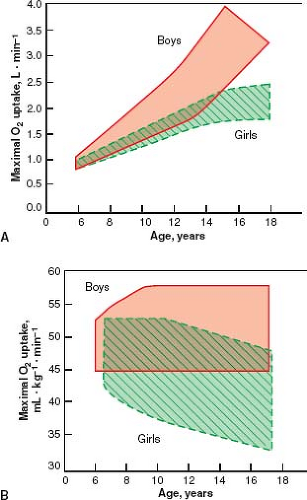 Figure 11.3 Part A (left) illustrates a composite graph of [V with dot above]O2max in absolute terms versus age in children; whereas part B (right) depicts the relationship with [V with dot above]O2max normalized for body mass. (From Bar-Or O, Rowland TW, eds. Pediatric Exercise Medicine—From Physiologic Principles to Health Care Application. Champaign, IL: Human Kinetics; 2004.) |
TABLE 11.2 Physiologic Changes Associated with Trained or Conditioned State | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
As demonstrated in Figure 11.6, resting heart rate decreases with improved fitness, and HRmax occurs at a higher [V with dot above]O2. It is apparent from this figure that submaximal heart rate is lower at any [V with dot above]O2 in the fit person compared with that in the unfit person. These adjustments of heart rate occur because of the increase in stroke volume that occurs with conditioning. Also, changes in the parasympathetic and sympathetic regulation of heart rate probably play an important role, with a relatively greater parasympathetic (vagal) influence on heart rate in the fit person. Changes in fitness or conditioning are not limited to changes in function of the cardiovascular system. The ventilatory changes listed are not the result of changes in resting lung function, but due to improved oxygen delivery and utilization thereby reducing ventilatory requirements in heavy exercise. Important changes also occur in subcellular changes in muscle and indeed, it is these changes that can contribute more to improved fitness with training. These are listed in Table 11.2. Fitness can be improved with regular episodes of sustained exercise. Conversely, deconditioning occurs if regular exercise is not done. Because children with heart disease may be sedentary, some component of reduced aerobic capacity in these patients may result from deconditioning.
Cardiac Responses to Acute Bouts of Exercise
Cardiac output is the product of heart rate × stroke volume. Cardiac output ([Q with dot above]) rises linearly with increasing [V with dot above]O2 (Fig. 11.4), as described by:
where k averages somewhere between 4 and 6 (24). The intercept, 4, is obviously somewhat dependent on the size of the subject, but is a good approximation for children within the “testable” age range (25). These relationships were obtained from steady-state exercise studies, but more recent work done during non–steady-state, progressive tests employing ramp or short-duration (e.g., 2-minute) step increments suggest this linearity may not be maintained.
Stringer et al. (26) demonstrated a noticeable leveling or plateau in the [Q with dot above] − [V with dot above]O2 relationship in four out of five subjects using invasive methods to measure [Q with dot above] during ramp exercise to voluntary exhaustion. Beck et al. showed that 38% of 72 healthy adults demonstrated nonlinearity in their [Q with dot above] − [V with dot above]O2 relationship during progressive exercise, and those subjects with higher [V with dot above]O2peak tended to exhibit a leveling of [Q with dot above] when plotted versus [V with dot above]O2 (27). Rowland recently demonstrated slight nonlinearity in the [Q with dot above] − [V with dot above]O2 relationship in preadolescent boys during progressive, maximal exercise with 3-minute increments, but the departure was so slight that one could still parsimoniously estimate a linear trajectory (28). The discrepancy between steady-state and non–steady-state behavior of the [Q with dot above] − [V with dot above]O2 function is likely the result of different time constants for [Q with dot above] than for [V with dot above]O2. In other words, if one of these variables reaches steady state more quickly than the other, there will be increasing divergence from the typical steady-state relationship of 4 to 6 L/min per L/min, eventually creating a curvilinear function when one plots [Q with dot above] versus [V with dot above]O2. Since time constants for HR and [V with dot above]O2 are faster in children than in adults, this nonlinearity may not be so evident in children. However, the dearth of data on kinetics of [Q with dot above] in children prevents one from drawing firm conclusions, and highlights deficits
in our understanding the dynamics of non–steady-state exercise in children.
in our understanding the dynamics of non–steady-state exercise in children.
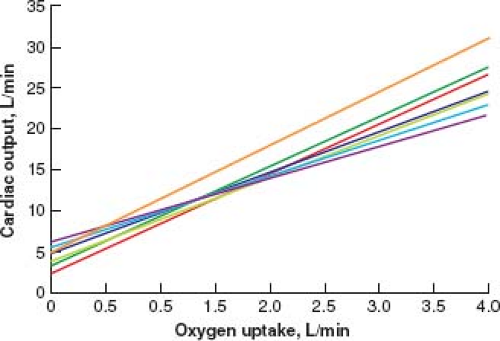 Figure 11.4 The relationship of cardiac output to oxygen uptake for normal persons. The various lines represent measurements from different laboratories using a variety of techniques for measuring cardiac output. |
Heart Rate
For normal persons, increased heart rate (HR) during exercise is the major determinant of increased cardiac output. There is a more or less linear relationship between heart rate and work. The “more or less” qualification is warranted because some children will show a lesser increment in HR with step changes in work at near-maximal exercise. Indeed, Godfrey et al. (25) have shown that a plot of HR versus logarithm [V with dot above]O2 yields a linear plot. It can be seen from Figure 11.5 that, in general, smaller children will have higher HR than larger children at any given work, and girls will have slightly higher HR than boys—particularly after puberty. Maximum heart rate (HRmax) that can be achieved is an important determinant of [V with dot above]O2peak, but will vary slightly depending on the exercise protocol used and the type of exercise performed. For example, a slightly higher HRmax is obtained for treadmill than for cycle exercise (29). For subjects between 5 and 20 years of age, HRmax is about 190 to 205 beats per min (bpm). HRmax for children younger than 5 years of age is likely similar, but it is difficult to motivate these youngsters to perform a truly maximal test. For subjects older than 20 years, predicted maximum heart rate is estimated according to the Astrand formula (220 – age) (30). The reasons for the decline of HRmax with age are unclear but may be related to fibrosis and scarring of the sinoatrial node. Heart rate reserve is defined as the difference between peak and resting heart rates, and has been shown to identify adults with congenital heart disease at higher mortality risk (31).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


