Nistri et al state that “in patients with hypertrophic cardiomyopathy without outflow obstruction at rest, the earlier onset of [left ventricular] outflow tract gradients during physiologic exercise was associated with impaired exercise performance. These findings provided insights into the determinants of functional impairment in [hypertrophic cardiomyopathy] and support the potential value of exercise echocardiography in the clinical assessment of patients with hypertrophic cardiomyopathy.”
We want to congratulate the investigators on their contribution to spreading the value of exercise echocardiography in the study of patients with hypertrophic cardiomyopathy. This elegant study is pioneering in the clarification of the influence of the moment of the appearance of obstruction during exercise in the functional capacity.
The results obtained by Nistri et al regarding the gradients at peak exercise in upright bicycle exercise and in the supine position differ from ours and from those of Dimitrow et al. We agree with the investigators’ explanation for these differences: the fact that in the studies cited, the patients were receiving active treatment with β blockers, verapamil, or both, “which could have substantially blunted the magnitude and altered the course of inducible obstruction.”
We disagree with Nistri et al when they state that “the present results, obtained during physiologic exercise and during pharmacologic ‘wash-out,’ have shown that it is equally acceptable to use either upright or post exercise supine technique to assess the magnitude of inducible obstruction in patients with hypertrophic cardiomyopathy for clinical purposes.”
It has been clearly shown that the magnitudes of gradients in patients with hypertrophic cardiomyopathy are higher in the upright position after exercise. We believe that these gradients are more accurate in reproducing the magnitude of inducible obstruction in real life.
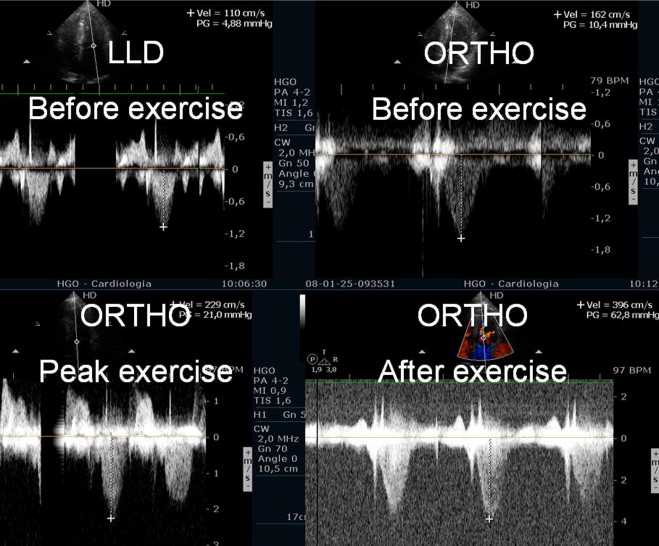
In our study, some of the patients with hypertrophic cardiomyopathy developed obstruction only after exercise in the orthostatic position ( Figure 1 ). The importance of upright evaluation after exercise termination was recently emphasized by Dimitrow et al. Usually, in real life, most patients who experience symptoms during or after exercise have them while standing up. So, it is logical that the evaluation of that phenomenon should occur in the same position to reproduce or better understand the physiopathology. Evaluation in the decubitus position would not be the most appropriate method in this scenario, although it is the current practice in most laboratories because of technical difficulties, which can be overcome with the proper operator training.