As with all clinical problems, it is essential to evaluate the patient thoroughly before considering management and treatment. If therapy is initiated before overall clinical evaluation has been performed, important clues may be obscured. Consider, for example, the patient with systemic arterial hypertension currently taking as simple a treatment as a thiazide diuretic. Associated metabolic changes may distort the clinical picture, including biochemical and cardiovascular risk factors (Table 2.1). This chapter considers important clues that may be obtained from a careful personal and family history, physical examination, and basic laboratory evaluation.
Table 2.1 Biochemical and other risk factors affecting patient evaluation when receiving a thiazide diuretic
Biochemical
Increased serum concentration of:
– Creatinine
– Glucose
– Cholesterol
– Uric acid
– Calcium
Decrease serum concentration of:
– Potassium
– Magnesium
Other risk factors
Diabetes mellitus
Hyperlipidaemia
Hyperuricaemia
Hypertension, curable causes
Elevated serum C-reactive protein
Family history
One striking feature of the concept of hypertension as a multifactorial disease is the presence of a strong family history of hypertension in some patients. When there is a family history of hypertension or of premature cardiovascular death, the likelihood of secondary forms of hypertension may be less (Table 2.2). However, should any of the secondary forms of hypertension be established, it is possible that the patient may also have essential hypertension, since the latter is present in about 20% of the overall population. Hence, it is important to search for and control other important cardiovascular risk factors, particularly in patients with a family history of premature death (Table 2.3). Should hypertension occur in both parents, there are additional considerations; since hypertension is a polygenetic disease, there is a greater likelihood that the disease may be more complex and severe.
Table 2.2 Clues suggesting a diagnosis of secondary hypertension
Absence of a family history of hypertension
Sudden onset of hypertension in a child or older adult
Sudden appearance of an elevated pressure when pressure had been well controlled previously
Appearance of refractoriness to previous effective antihypertensive therapy
Physical examination findings or abnormal laboratory findings suggestive of a secondary cause of hypertension
Table 2.3 Important factors in the family history
Family history of premature death from
Myocardial infarction
Heart failure
Stroke
Kidney failure
Coexistent risk factors with hypertension
Atherosclerosis
Obesity
Diabetes mellitus
Hypercholesterolaemia or other hyperlipidaemias
Gout
Smoking
Physical inactivity
Microalbuminuria
Age (male ≥55 years; female ≥65 years)
Black race
Clinical history
In most patients with systemic hypertension there are generally no clinical manifestations other than elevated systolic and/or diastolic pressures. Therefore, unless blood pressure is measured in all patients, hypertension will remain unrecognized and untreated, and there will be no further improvement in the control rates of hypertensive disease in any given population.
The most common symptoms traditionally related to hypertension have been fatigue, headache and epistaxis, but these symptoms are among the most common complaints offered by any patient seeking medical attention. However, when other symptoms are present, they are more likely to be related to the ‘target organ’ (i.e. heart, kidneys, brain) of the disease (Table 2.4). In this regard, it is important to question the more subtle signs so that the correct diagnosis can be made for those patients with earlier stage 1 hypertension.
Table 2.4 Symptoms of hypertension related to target organ involvement
Brain
Transitory episode(s) of sensory or motor deficit
Dizziness, fainting, vertigo
Sudden loss of vision (total or part of visual field)
Hypertension cannot be controlled and its complications cannot be prevented if blood pressure is not routinely measured and properly obtained during every physical examination. This should be done by all primary care physicians, specialists, dentists and other health care professionals. However, it is important to emphasize that the diagnosis should not be made on the basis of any single measurement. Repeated measurements should be obtained during each individual examination, and the diagnosis is established if these blood pressure measurements are made two or three times, and were elevated on three successive office visits (including the first). The American Heart Association, the Joint National Committee and the World Health Organization have all recommended similar follow-up procedures for repeated measurements based upon the initial measurements.
Table 2.5 Procedure for the indirect measurement of blood pressure
Patients should be seated with the arm bared, supported, and at heart level. The patient should not have smoked or ingested caffeine within 30 minutes before measurement
Measurement should begin after at least 5 minutes of rest. The appropriate cuff size must be used to ensure an accurate measurement. The cuff bladder should nearly (at least 80%) or completely encircle the arm
Measurements should be taken with a mercury sphygmomanometer, a recently calibrated aneroid manometer or a calibrated electronic device
Both the systolic and diastolic pressure should be recorded. Disappearance of sound (phase V) should be used for the diastolic reading
Two or more readings separated by 2 minutes must be taken and an average reading obtained. If the first two readings differ by >5 mmHg, additional readings must be obtained
In addition, blood pressure must be measured in both arms on the initial physical examination and periodically thereafter. It is not unusual that the measured pressure will be reduced over several years from the initial examination in those elderly patients with occlusive brachial arterial disease
During the procedure the patient and examiner should refrain from talking
These recommendations advise use of a systematic technique (Table 2.5) and additionally advise on the purpose and meaning of blood pressure measurements, with specific recommendations on follow-up. Furthermore, should the patient assist in follow-up with home blood pressure measurements, the instrument must be calibrated and validated periodically (at least once annually). There is no part of the physical examination on which the diagnosis of hypertension is more dependent than the precise and repeated measurement of blood pressure.
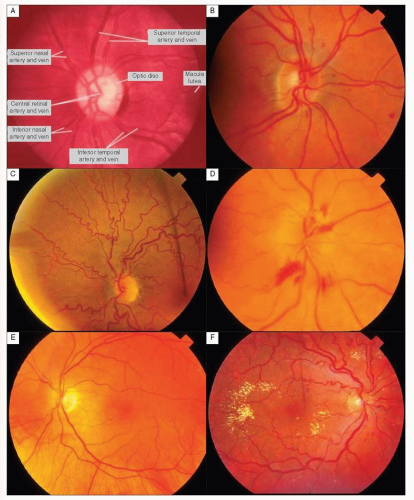
Ophthalmoscopy
The small vessels of the optic fundus provide an excellent means for assessing the degree of systemic vasoconstriction (2.1A-F). This examination should be performed routinely. The earliest stage (group 1) of hypertensive vascular disease is recognized by increased tortuosity and mild constriction of the vessels. Coexisting sclerotic changes are manifested by the discontinuity of the vessels at the arteriovenous (AV) crossings (i.e. AV nicking (group 2)(2.1B). The appearance of exudates and haemorrhages (group 3) signals accelerated hypertension; and with the appearance of papilloedema (group 4), malignant hypertension is established (2.1C-F).
The American Ophthalmological Association has offered a more detailed classification based upon the degree of narrowing of both the retinal arterioles and venules (Table 2.6).
Peripheral pulses
The femoral and brachial arterial pulsations in all patients with hypertension must be compared in order to search for any delay in the propagation of the aortic pulse wave, suggesting the presence of aortic coarctation (particularly in younger patients). Although this diagnosis should be considered in all patients, including adults, it may also suggest an atherosclerotic occlusive process in the elderly, particularly if there are asymmetrical brachial arterial pressures or if, on long-term follow-up, there is an unexplained reduction in pressure taken in one arm, or a reduction or loss of peripheral pulsations. If that occurs, pressure should be measured in the contralateral arm, and further evaluation can be done for occlusive vascular disease.
Auscultation of the carotid arteries for systolic bruits may provide signs of preventable strokes and transient ischaemic attacks (especially if associated with neurological signs and symptoms). It is important to dissociate bruits heard over the carotid arteries from transmission of aortic systolic ejection-type murmurs. This usually can be clarified by listening carefully for the timing and character of the bruits. Furthermore, funduscopy may reveal cholesterol emboli in the retinal arterioles. Renal arterial bruits on examination of the abdomen, flanks and back provide an important sign of renovascular hypertension. Systolic bruits are more commonly detected, especially in older patients, and may not be associated solely with occlusive renal arterial disease. However, when the abdominal bruit is associated with a diastolic component in the upper quadrants of the abdomen or flanks, the possibility of renal arterial disease becomes much more likely and should be focused on.
2.1 Fundoscopy in hypertension. A: normal funduscopic examination demonstrating vessels and the optic nerve head; B: severe arteriolar constriction; C: marked arteriolar tortuosity; D: marked arteriolar constriction and flame-shaped haemorrhages; E: accelerated hypertension with severe arteriolar constriction, haemorrhages and exudates; F: malignant hypertension with severe arteriolar constriction and tortuosity, haemorrhages, exudates and papilloedema.
Table 2.6 Classification of hypertensive retinopathy
Keith-Wagener-Barker classification
Group I — tortuosity, minimal constriction
Group II — as above + arteriovenous nicking
Group III — as above + haemorrhages and exudates
Group IV — papilloedema
American Ophthalmological Society Committee Classification (Wagener-Clay-Gipner) Generalized arteriolar constriction:
Grade 1 — arterioles ¾ of normal calibre; AV ratio of 1:2
Grade 2 — arterioles ½ of normal calibre; AV ratio of 1:3
Grade 3 — arterioles 1/3 of normal calibre; AV ratio of 1:4
Grade 4 — arterioles thread-like or invisible
Focal arteriolar constriction or sclerosis
Grade 1 — localized arteriolar narrowing to 2/3 calibre of proximal segment
Grade 2 — localized arteriolar narrowing to ½ calibre of proximal segment
Grade 3 — localized arteriolar narrowing to 1/3 calibre of proximal segment
Grade 1 — increased light-striping; mild AV nicking
Grade 2 — coppery arteriolar colour; moderate AV nicking; veins almost completely invisible below arteriolar crossing
Grade 3 — silver arteriolar colour; severe AV nicking
Grade 4 — arterioles visible only as fibrous cords without bloodstreams
Haemorrhage and exudates
Grades 1 to 4 (based on the number of affected quadrants divided by 2)
Papilloedema
Grades 1 to 4 (based on dioptres of elevation)
Cardiac examination
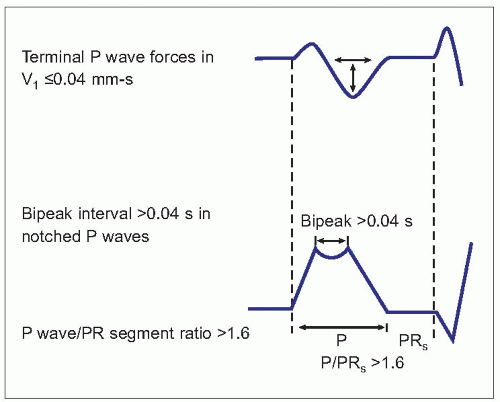
Even before cardiac structure is altered (particularly in young patients), precordial palpation may reveal evidence of functional hyperdynamic cardiac changes, namely hyperdynamic apical impulse and a faster heart rate. As the heart adapts structurally to the increasing afterload by development of left ventricular hypertrophy (LVH), increased ventricular mass may be suspected by a sustained apical lift although it may not be detectable by the chest roentgenogram. The electrocardiogram and echocardiographic assessment are more sensitive. Nevertheless, the earliest clinical index of cardiac involvement in hypertension is left atrial enlargement, which may be suspected by an atrial diastolic gallop (fourth heart sound or the bruit de gallop). This finding is highly concordant with at least two of four electrocardiographic criteria of left atrial abnormality (Table 2.7, 2.2).
Haemodynamic and echocardiographic studies have demonstrated that when electrocardiographic evidence of left atrial abnormality is present (even without other indications of LVH), there is adequate evidence of impaired left ventricular (LV) systolic function. As LVH becomes more evident clinically, as indicated above, there is palpable evidence of a sustained LV lift (or ‘heave’) and further impairment of contractile function. In patients with severe LVH, the presence of a third heart sound (ventricular diastolic gallop) eventually connotes the presence of early LV failure. In those patients with a very high arterial pressure, an aortic diastolic ‘blowing’ murmur may occur as the result of a functional eversion of the aortic cusp by elevated pressure and total peripheral resistance. The more frequently heard precordial or vascular systolic ejection murmur suggests either outflow tract obstruction from (absolute or relative) aortic stenosis (associated with ageing), or a haemic murmur related to a hyperkinetic circulation or coexistent anaemia.
Other physical findings
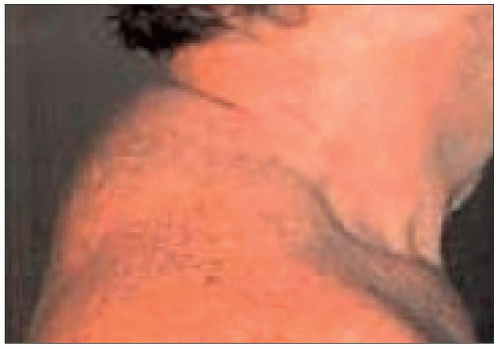
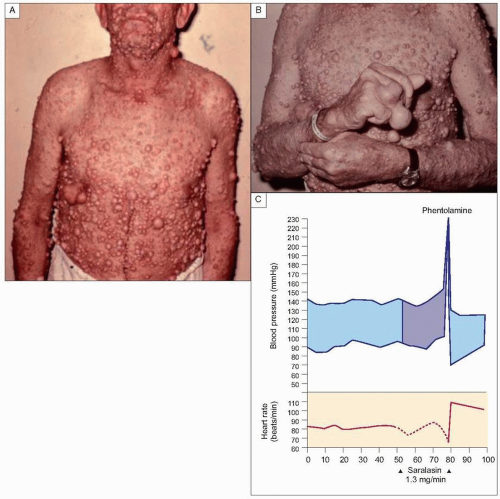
The so-called ‘buffalo hump,’ seen on the back below the neck, suggests Cushing’s syndrome (2.3). This may also be associated with abdominal striae and girdle obesity. Neurofibromatosis or café-au-lait skin spots can suggest possible coexistent phaeochromocytoma (2.4A-C). In the days prior to effective antihypertensive therapy, cutaneous ulcerations were seen as manifestations of severely impaired cutaneous blood flow (2.5). Appearance of anaemia on physical examination in the black patient should suggest coexistent haemoglobinopathy or anaemia secondary to chronic renal disease. Careful abdominal examination is necessary for the auscultation of bruits, as well as for the presence of the palpable kidneys of polycystic kidney disease (PKD). When the latter occurs, hepatic cysts, secondary polycythaemia and cerebral aneurysmal disease of the circle of Willis should also be considered.
2.2 Electrocardiographic criteria for left atrial abnormality.
2.3 Buffalo hump.
2.4 Neurofibromatosis. A, B: skin lesions; C: patients may also have a phaeochromocytoma. When the angiotensin II anatagonist saralasin is infused it stimulates the release of catecholamines from the phaeochromocytoma. Medullary blood pressure is reduced with administration of the adrenergic antagonist phentolamine. The phaeochromocytoma was subsequently surgically removed.
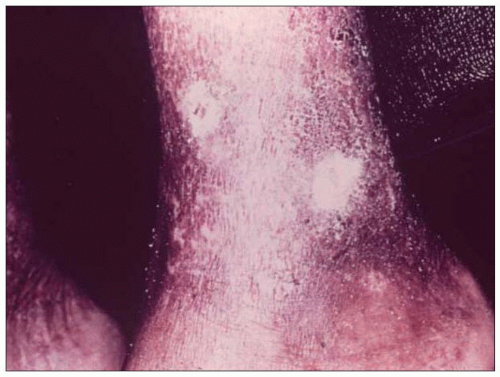
2.5 Hypertension-related cutaneous skin ulceration. The lesion was slow healing but improved with blood pressure control.
Laboratory studies
It is important to discuss with the patient appropriate preparation for laboratory tests, including cessation of all medication, preferably for at least 2 weeks (Table 2.8). Even a sodium-restricted diet may stimulate adrenal cortical production of aldosterone in sufficient quantities to suggest a state of hyperaldosteronism. Dietary sodium intake in excess of 100 mmol (mEq)/day (2.3 g), will obviate this possibility. This degree of restriction of daily sodium intake may still be effective, either in reducing pressure in some patients or in enhancing effectiveness of the antihypertensive drugs.
It is important to realize that diuretics, laxatives and intercurrent gastrointestinal problems (associated with nausea, vomiting and diarrhoea) may incur sufficient volume depletion and electrolyte loss so as to produce evidence of secondary hyperaldosteronism with associated hypokalaemia and alkalosis. Some antihypertensive drugs may have effects lasting for several weeks, thereby providing a false concept of ‘baseline’ untreated pressure levels. For example, the thiazide diuretics may have persistent effects for 2 weeks following discontinuation. Oral contraceptives may elevate arterial pressure and alter intravascular volume, haemodynamics and plasma renin activity. Certain ‘street drugs’ (e.g. heroin, cocaine) will elevate blood pressure; hence, it is important to obtain an accurate history of all medications or over-the-counter drugs that the patient is taking.
Certainly, not all studies discussed below may be necessary in evaluating all patients; however, this discussion provides a means for understanding overall laboratory evaluation. The minimal evaluation is presented in Table 2.9. The fewer the laboratory studies, the more cost-effective the evaluation will be. However, modern automated laboratory testing techniques provide more measurements and thus a more comprehensive evaluation, frequently at no greater cost.
Complete blood count (CBC)
In addition to assessing the haematological status of the patient, the CBC has broader significance and importance. If anaemia is present, the physician should determine whether it is a complication of the disease, a side-effect of drug therapy or a result of a coexistent disease (Table 2.10). An elevated haemoglobin concentration or haematocrit frequently occurs in patients with essential hypertension (see Gaisböck syndrome, Chapter 1). It is also of value to know pretreatment white blood cell count, since leucopenia may complicate angiotensin-converting enzyme (ACE) therapy. Thus, a baseline haemogram determination may be of great value for future care.
Table 2.8 Laboratory tests for the evaluation hypertension
Blood studies
Complete blood count
White blood cell count (and differential)
Haemoglobin concentration
Haematocrit
Adequacy of platelets
Blood chemistries
Glucose (fasting, 2-hour postprandial, or glucose tolerance test, as indicated)
Uric acid concentration
Cholesterol (total and with high- and low-density lipoprotein fractions) and triglyceride concentrations
Renal function (serum creatinine and/or blood urea concentrations)