Evaluation of Quality of Life in Children and Adolescents with Congenital and Acquired Heart Disease
Bradley S. Marino
Introduction
Due to recent advances in pediatric cardiovascular therapy, mortality rates for children with heart disease (HD) have decreased dramatically. Despite these advances, however, survivors suffer from morbidity resulting from their circulatory abnormalities and the medical and surgical therapies that they have received. These morbidities significantly impact the child’s neurodevelopmental, psychosocial, and physical functioning and diminish their quality of life (QOL). As a result, outcome assessment focusing on QOL has become increasingly important in this high-risk population. QOL may be described as a child’s ability to function in situational contexts and derive personal satisfaction from doing so.
Ultimately, the goals of pediatric research and clinical care are to maximize health and minimize symptomatology, disability, and dysfunction that may impact the lives of children who have acute and chronic disease processes. Over the last several decades, new surgical techniques and advances in cardiopulmonary bypass, intensive care, interventional cardiac catheterization, noninvasive imaging, and medical therapies have significantly lowered neonatal mortality rates for children with the most complex congenital heart disease (CHD) (e.g., hypoplastic left heart disease) to less than 10% (1). In addition, cardiac-related mortality in patients with congenital and acquired HD has diminished significantly during the first two decades of life (2,3). Although survival rates vary by disease complexity, long-term survival (>20 years) rates for children with CHD are estimated to be 95% for simple CHD, 90% for moderate CHD, and 80% for complex CHD in the current era (3).
Despite these advances, however, survivors suffer from morbidity resulting from their circulatory abnormalities and the medical and surgical therapies that they have received. These morbidities significantly impact the child’s neurodevelopmental (4,5,6), psychosocial (7,8,9), and physical (10,11,12) functioning and diminish their QOL (Fig. 77.1). Given the high incidence of functional impairment in the pediatric cardiac population, there has been a paradigm shift in clinical research from prevention of short-term mortality to long-term assessment of morbidity. As a result, outcome assessment focusing on QOL has become increasingly important in this high-risk population.
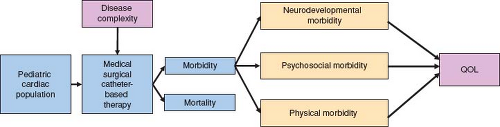 Figure 77.1 The relationship between heart disease-related morbidity factors and QOL. (From Marino BS, Uzark K, Ittenbach I, Drotar D. Evaluation of quality of life in children with heart disease. Prog Ped Cardiol. 2010;29:131–138, with permission.) |
QOL may be described as a child’s ability to function in situational contexts (family, school, and peer) and derive personal satisfaction from doing so (13,14,15). The multidimensional construct of QOL is thought to include three essential domains: physical health status and physical functioning; psychological status, and social functioning (Fig. 77.2) (13,14,15). QOL measurement provides a comprehensive description of an individual’s health, may result in the identification of physical, functional, and psychosocial dysfunction, and is a critical component of the evaluation of long-term outcomes of chronic conditions and disease-specific therapies.
This chapter will delineate health-measurement definitions including QOL and health-related QOL (HRQOL), identify inherent difficulties in HRQOL measurement in the pediatric HD population, and discuss salient aspects of HRQOL evaluation. In addition, it will describe existing generic and disease-specific HRQOL measures that may be used to assess HRQOL in the pediatric HD population, what research on HRQOL in the pediatric HD population has shown, and the extent to which HRQOL evaluations are being fully utilized in clinical practice. Finally, a research and clinical agenda is proposed to harness the potential applications of HRQOL assessment.
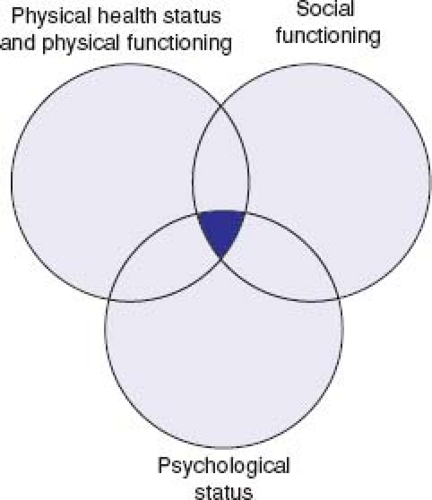 Figure 77.2 Definition of quality of life. (From Marino BS, Uzark K, Ittenbach I, Drotar D. Evaluation of quality of life in children with heart disease. Prog Ped Cardiol. 2010;29:131–138.) |
Health Measurement Definitions: QOL and HRQOL
There are many ways to define “health.” While the differences in meaning between various attributes of health may be subtle, the differences are important and have significant implications as to how clinical and research data are interpreted and findings incorporated into how we care for children with chronic disease. Health has been defined by the World Health Organization as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (16). Indeed it was this initial definition of health that gave rise to the concept of QOL. Health status, which impacts QOL, may be thought of as a child’s level of wellness versus illness, describing the impact of physiologic dysfunction, symptom burden, and/or level of illness control. Alternatively, functional status is defined as an individual’s ability to perform activities of daily living, meet basic needs, fulfill roles, and maintain health and well-being within the context of various life situations (17). Functional status is often affected by health status and has a significant impact on QOL. However, it is HRQOL, a more specific description of QOL, which is the most relevant construct relative to clinical and research data assessing outcomes and the provision of comprehensive clinical care of children and adolescents with chronic illness or injury (18). HRQOL is defined as the influence of a specific illness, medical therapy, or health services policy on the ability of the patient to both function in and derive personal satisfaction from various physical, psychological, and social life contexts (19). For the purposes of this manuscript all references to QOL hereafter are referring specifically to HRQOL.
Evaluating HRQOL is important because it allows better communication among patients, parents, and healthcare providers, prioritization of problems based partially on patient and/or parent preference, monitoring of changes over time or in response to a specific therapy and screening for other significant physical and psychosocial problems (20). HRQOL measurement has emerged as a high priority not only for patients, their families and medical caregivers, but also for the National Institutes of Health (NIH), Food and Drug Administration (FDA), and insurance providers (21). The NIH’s Patient-Reported Outcomes Measurement Information System, part of the NIH Roadmap, is a multimillion-dollar effort devoted in part to improving HRQOL (22,23,24,25,26,27). The FDA recognized the importance of such patient-reported outcomes by issuing guidance to industry on the use of such outcomes in clinical trials in support of medical product efficacy (28). A better understanding of the perceptions of HRQOL among patients with HD, and their parents and healthcare providers may improve treatment and patient outcome (29,30) and the ability to perform important prospective cross-sectional, cohort, and randomized clinical trials to improve patient outcome. Despite the known advantages, assessment of HRQOL in the pediatric cardiac population is lacking.
Measurement of HRQOL in patients with congenital and acquired HD has been limited over the last 25 years. Moons et al. (31) noted that only 1 of 70 studies published between 1980 and 2003 that purported to assess HRQOL in pediatric cardiac patients actually measured the patient-perceived HRQOL. In addition, more than half of the 70 articles did not meet any of the 10 critical appraisal criteria for HRQOL research studies advocated by Gill and Feinstein in JAMA in 1994 (32). The lack of rigorous research on HRQOL in the pediatric HD population is not surprising, given the inherent difficulties of measuring HRQOL in this population.
Inherent Difficulties of HRQOL Evaluation in the Pediatric HD Population
HRQOL assessment in the pediatric population is challenging due to the wide age range and the changing developmental capabilities of patients as they age. HRQOL assessment in the pediatric cardiac population is further complicated by the variety of congenital and acquired diseases, varying levels of severity, the array of therapeutic modalities that may be utilized to treat the patient (medical, surgical, and interventional), and the spectrum of outcomes. Similar to other pediatric chronic diseases, there may be variation in the perceived impact of HD on HRQOL, as many of the patients have always had HD (congenital HD) while others have been diagnosed with HD at an age when they were aware of the acute change in their health status (acquired HD).
Patient-family interactions are critical in QOL assessment, and the role of proxy-reporting (parent/guardian) and cross-informant variance is often debated (33). It has been extensively documented that HRQOL measurement in children with chronic health conditions and healthy children provided by proxy-respondents is not equivalent to that reported by the child (34,35). These findings indicate that proxy-reports cannot be substituted for children’s self-reports (36) and evaluations of pediatric cardiac patients’ own perspectives regarding treatment outcomes should be included in pediatric clinical care and clinical trials given the documented differences between child and proxy-reports. While pediatric patient self-reporting should be considered the standard for measuring patient-perceived HRQOL (37), there may be situations when the child is too young, too cognitively impaired, or too ill to complete an HRQOL instrument, and proxy-reporting may be required. Further, it is typically parents’ perceptions of their child’s HRQOL that influences healthcare use (38,39). Ideally, parent and child QOL instruments should be chosen that measure the perspectives of both the child and proxy-reporter within the same constructs and use parallel items to make comparisons between self- and proxy-reports more informative and useful (40). As noted by Moons et al. (31) most studies assessing HRQOL in children with HD have only assessed proxy-reporters (parents/guardians) and have ignored the perceptions of the child. Studies of the cognitive development in children, psychometric studies on QOL measures that have included child self-reporting, and cognitive-interviewing studies on children’s abilities to respond to questionnaires indicate that self-reports from children over 7 years of age are reliable and valid (41).
Both patients and their parents provide important information, even though they may vary or even disagree significantly with one another. Marino et al. demonstrated that pediatric patients with HD and their parents identify similar items of importance relative to QOL assessment, which differs from those described by physician and nurse providers (30). In addition, Costello et al. showed that
clinicians (intensive care and outpatient cardiologists and cardiovascular nurses) performed poorly when asked to predict HRQOL for children with cardiac disease (42). Healthcare providers in pediatric cardiology should be cognizant of these data when providing counseling and incorporate multiple-informant assessment of QOL into their practices. Considering the QOL perceptions of the patient and family may help guide individualized decision-making about treatment and allow the clinician to maximize the long-term psychosocial, physical, and ND outcomes of their patients with HD. It may be that understanding the differences in perception of HRQOL between patients, their parent/guardians, and medical caregivers may be more important and informative than perceived agreement (30).
clinicians (intensive care and outpatient cardiologists and cardiovascular nurses) performed poorly when asked to predict HRQOL for children with cardiac disease (42). Healthcare providers in pediatric cardiology should be cognizant of these data when providing counseling and incorporate multiple-informant assessment of QOL into their practices. Considering the QOL perceptions of the patient and family may help guide individualized decision-making about treatment and allow the clinician to maximize the long-term psychosocial, physical, and ND outcomes of their patients with HD. It may be that understanding the differences in perception of HRQOL between patients, their parent/guardians, and medical caregivers may be more important and informative than perceived agreement (30).
In addition to issues related to the assessment of the pediatric population in general and the pediatric HD population specifically, issues related to cultural and demographic variables (culture, race, ethnicity, income) also affect HRQOL assessment in both pediatric and adult respondents. Culture, race, ethnicity, and income have critical influences on HRQOL measurement relative to the values that are attributed to various health states by children and their parents, the language in which health is described by children and their families, and the perceived functional impact of symptoms and changes in health states (43).
HRQOL Instrument Evaluation
When measuring HRQOL it is important to be clear on whether the goal of the application is to assess HRQOL or functional status or both. These measures of health are distinct constructs and are often confused with each other (note prior definitions). When assessing either HRQOL or functional status for research and clinical application, specific aspects of instrument selection (Tables 77.1 and 77.2), validation (Table 77.3), and availability (Table 77.4) must be considered.
When selecting an instrument it is important to note the instrument type, the specific construct that will be assessed, the desired respondent type(s), patient and proxy-reporter age range(s), and the domains to be assessed (see Table 77.1). When selecting a specific form from within an instrument grouping, the number of items in the tool and the average completion time should be considered as they may impact the feasibility of completing the research project or clinical application (see Table 77.2).
Both generic and disease-specific instruments exist that may be used to measure HRQOL or functional status in the pediatric HD population (44,45,46,47,48,49,50). Whether generic or disease-specific, the “ideal” QOL measure would have a patient self-reporting mechanism with parent/guardian proxy-reporting, applicability to a wide age range, would be easily self-administered in a reasonable timeframe, and would have an array of relevant constructs to describe and measure HRQOL or functional status. Generic HRQOL or functional status measures assess these constructs in both healthy children and in children with chronic disease. They may be used to compare various chronic disease groups or chronic disease groups and healthy controls. Disease-specific instruments assess HRQOL in a particular condition or disease, may be more comprehensive for a specific disease, and may be better discriminators of differences between subgroups within a disease category. Disease-specific pediatric cardiac HRQOL instruments may provide new, critical information on the outcome of present and future interventional catheterization and cardiac surgical procedures in the short and long term and may be utilized for randomized clinical trials for cardiovascular drugs and new technologies and interventions. Ideally, a disease-specific pediatric cardiac HRQOL instrument would define changes in HRQOL over time (evaluative tool), predict future changes in HRQOL (prognostic tool), and signal new problems or issues that might not be noted by traditional biologic markers (diagnostic tool).
Assessing prior validation data on a given HRQOL or functional status instrument is central to evaluation of the instrument (see Table 77.3). When validating a given instrument, four specific questions relative to the psychometric properties of the instrument should be asked: (1) Has the instrument been shown to be reliable in the patient population being studied?; (2) Has the instrument been shown to be internally valid in the patient population being studied?; (3) Has the instrument been shown to be externally valid in the patient population to be studied?; (4) If the study is assessing change over time or the impact of an intervention, has the instrument been shown to be responsive in the patient population to be studied?
All psychometric instruments must be shown to be reliable before validity and responsiveness may be considered (51). An “unreliable instrument” cannot be deemed valid or responsive. Demonstrating reliability involves assessing score “reproducibility” through internal consistency measurement (Cronbach α) and comparing scores on the same patient at two distinct points in time with an appropriate interval between them to minimize recall bias (test–retest reliability). Testing the validity of a psychometric scale is an ongoing, evidence-based process that assesses the degree of confidence one should have in inferences made about a test-taker based on their score. Assessing validity is often divided into the domains of “internal” and “external” construct validity (52,53,54). “Internal validity” (51,53,55) may be thought of as an assessment of content validity and structural validity, which includes an assessment of the theoretical conceptualization of the respective instrument, the clarity, relevance, and representativeness of the item content and tool construction. In contrast, establishing “external validity” requires demonstrating convergent and discriminant construct validity and “generalizability” (52,53,56). “Generalizability” may be defined as the ability of a tool to provide valid and reliable information when utilized in different geographic regions and patient populations (53). Generalizable tools allow researchers to have confidence that data collected from multiple sites and regions are comparable. Substantiation of the “generalizability” part of external validity enables an HRQOL instrument to be used for clinical applications and multicenter research that may serve as a platform for future multisite cross-sectional and prospective studies using HRQOL as an outcome. Responsiveness describes the ability of the instrument to be sensitive to change in score after intervention or to meaningful changes over time if a patient’s health status or functional status alters (51). Having a responsive instrument is critical to any interventional agenda or follow-up program for any given chronic disease population.
Existing Generic and Disease-Specific HRQOL Measures that may be Used to Assess HRQOL in the Pediatric HD Population
The PedsQL 4.0 Core Scale, a generic HRQOL measure, and the Child Health Questionnaire (CHQ), a generic functional status measure, have patient and proxy-reporting, are applicable to a wide age range, and may be administered in a reasonable timeframe. In addition, these commercially available tools have been shown to be reliable, internally and externally valid, responsive and applicable in many other countries after language translation (see Tables 77.1 to 77.4) (44,45). Five disease-specific pediatric cardiac HRQOL instruments have been previously described (46,47,48,49,50). The Congenital Heart Disease-TNO/AZL Adult QOL (CHD-TAAQOL) questionnaire is a disease-specific instrument that assesses HRQOL in young adults with CHD (46). The PedsQL 3.0 Cardiac Module (47), Congenital Heart Adolescent and Teenager Questionnaire (CHAT) (48), ConQol (49), and Pediatric Cardiac Quality of Life Inventory (PCQLI) (50) measure HRQOL in the pediatric cardiac population. Instrument availability (form specific authorization requirements, user costs, and available language translations) is shown in Table 77.4. The PedsQL 3.0 Cardiac Module (47), created and validated by Uzark et al. at a single site, was a critical and important step forward in the objective assessment of HRQOL in children with HD. The PedsQL 3.0 Cardiac Module has been shown to be reliable, internally and
externally valid. The 27-item PedsQL Cardiac Module encompasses six scales: Heart Problems and Treatment, Treatment II, Perceived Physical Appearance, Treatment Anxiety, Cognitive Problems, and Communication (47,57). The PedsQL 3.0 Cardiac Module has not yet been shown to be generalizable to other geographic regions or demographic populations in the United States. The CHAT and ConQol questionnaires have important limitations that include their intended use for HD patients with CHD only (48,49), applicability to a narrow age range (48,49), a lack of parent proxy-reporting (49) and no generalizability data to support their broad applicability to other geographic regions or demographics within the United States (48,49), and/or an inadequate ability to discriminate among various types of cardiovascular disease across a wide age range (49). The PCQLI is the most recently published disease-specific instrument. Similar to the PedsQL 3.0 Cardiac Module, it has a patient self-reporting mechanism with parent/guardian proxy-reporting, wide age range, which is easily self-administered in a reasonable time-frame, and has an array of relevant constructs to describe and measure HRQOL in the pediatric HD population. The PCQLI is the only disease-specific measure that has been tested in a multicenter trial and shown to be reliable, valid, and generalizable in the United States (58,59). The ConQol and PedsQL 3.0 Cardiac Module can distinguish among disease severity subgroups but only within select subsets of a study population (age, respondent type) (47,49). In contrast, PCQLI Total and subscale scores (Disease Impact and Psychosocial Impact) differentiate between congenital HD severity subgroups irrespective of age category, score examined or respondent type (40). From a research perspective, this is an important development that will facilitate cross-sectional and prospective studies of HRQOL in clinically important subgroups in the pediatric HD population. It is important to note that none of the five disease-specific instruments has been shown to be responsive in the United States.
externally valid. The 27-item PedsQL Cardiac Module encompasses six scales: Heart Problems and Treatment, Treatment II, Perceived Physical Appearance, Treatment Anxiety, Cognitive Problems, and Communication (47,57). The PedsQL 3.0 Cardiac Module has not yet been shown to be generalizable to other geographic regions or demographic populations in the United States. The CHAT and ConQol questionnaires have important limitations that include their intended use for HD patients with CHD only (48,49), applicability to a narrow age range (48,49), a lack of parent proxy-reporting (49) and no generalizability data to support their broad applicability to other geographic regions or demographics within the United States (48,49), and/or an inadequate ability to discriminate among various types of cardiovascular disease across a wide age range (49). The PCQLI is the most recently published disease-specific instrument. Similar to the PedsQL 3.0 Cardiac Module, it has a patient self-reporting mechanism with parent/guardian proxy-reporting, wide age range, which is easily self-administered in a reasonable time-frame, and has an array of relevant constructs to describe and measure HRQOL in the pediatric HD population. The PCQLI is the only disease-specific measure that has been tested in a multicenter trial and shown to be reliable, valid, and generalizable in the United States (58,59). The ConQol and PedsQL 3.0 Cardiac Module can distinguish among disease severity subgroups but only within select subsets of a study population (age, respondent type) (47,49). In contrast, PCQLI Total and subscale scores (Disease Impact and Psychosocial Impact) differentiate between congenital HD severity subgroups irrespective of age category, score examined or respondent type (40). From a research perspective, this is an important development that will facilitate cross-sectional and prospective studies of HRQOL in clinically important subgroups in the pediatric HD population. It is important to note that none of the five disease-specific instruments has been shown to be responsive in the United States.
TABLE 77.1 Instrument Selection: Constructs, Respondent Types, and Domains | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 77.2 Instrument Selection: Forms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


