Epiphrenic Diverticulum
Presentation
A 64-year-old man presents with a 4-month history of solid food dysphagia associated with a 12-pound weight loss. He also complains of excessive belching and regurgitation within 1 hour of meals. He reports a 40-pack-per-year smoking history and no history of alcohol abuse. He presents with a chest x-ray that was obtained by his primary medical physician.
▪ Chest X-ray
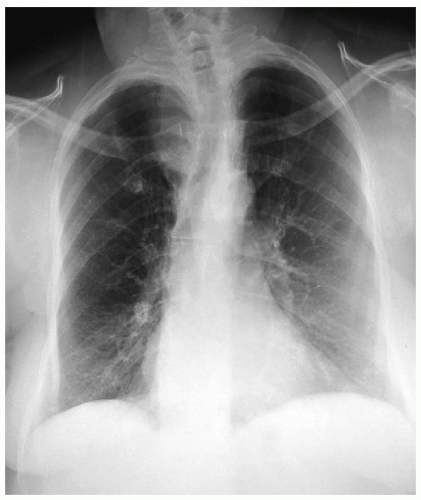 Figure 3-1 |
Chest X-ray Report
There are no lung masses or pleural effusions. The trachea is shifted to the right. The heart size is normal.
Discussion
The differential diagnosis for dysphagia includes obstructive etiologies as well as etiologies from neuromuscular disorders. Obstructive etiologies include causes such as cancer of the esophagus, Schatzki’s ring, peptic strictures, and webs. Neuromuscular etiologies include achalasia, diffuse esophageal spasm, and the nutcracker esophagus. Other rare etiologies of dysphagia include those associated with extrinsic compression of the esophagus, such as with aberrant vasculature, lymphadenopathy, and medi as ti nal masses.
The history and physical examination are important in evaluating patients for dysphagia. Many of the signs and symptoms that can be elicited from the patient by careful and detailed history and physical examination will aid in determining the most likely diagnosis. An upper gastrointestinal (GI) study provides an excellent diagnostic evaluation for patients who present with dysphagia and symptoms of esophageal obstruction. This study also provides some information on esophageal motility. A double-contrast study better demonstrates esophageal mucosa. Other studies, such as endos copy, manometry, and 24-hour pH monitoring, may be needed after upper GI studies demonstrate an esophageal pathology.
▪ Upper GI Studies
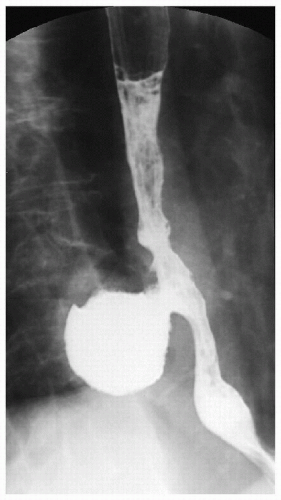 Figure 3-2 |
 Figure 3-3 |
Upper GI Study Report
There is a 5-cm × 5-cm epiphrenic diverticulum with a 2-cm orifice. Fluoroscopy reveals tertiary contractions within the esophagus. Gastroesophageal reflux, to the level of the thoracic inlet, is also demonstrated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


