Chapter 14 Endovenous Thrombectomy and Thrombolysis
Historical Background
After the first episode of deep venous thrombosis (DVT), affected patients may develop pulmonary embolism (PE), recurrent DVT, or postthrombotic syndrome (PTS), and all carry significant morbidity and negative socioeconomic impact.1 Important concepts in the natural history of the disease are recurrence, propagation, and recanalization with anatomic and/or hemodynamic changes following an episode of DVT. Spontaneous resolution of the DVT leaving intact the affected segment is rarely found, occurring only in one-third of patients.2 Frequently, the segment affected by thrombosis develops reflux due to venous valve injury or some degree of residual obstruction.3 Patients who develop a combination of reflux and venous obstruction following an episode of DVT have the highest risk of developing PTS.3,4 A combination of reflux and obstruction is found in up to 86% of the patients, while occlusion alone is found in less than 10%.5
Patients with extensive proximal DVT, such as iliocaval or iliofemoral occlusions, have a worse prognosis compared with patients with infrainguinal thrombosis.6,7 The resolution of venous obstruction with iliac thrombosis is often incomplete, and the incidence of PTS is higher.4 Recurrent DVT is a very important factor in the natural history of the disease because other than exposing the patient to PE, it also increases significantly the risk for developing PTS.8 In fact, it has been shown that a recurrent ipsilateral DVT is the strongest predictor for developing skin damage.9 The risk of recurrent DVT was 40% (95% confidence interval [CI], 35.4% to 44.4%) after 10 years, being 53% (95% CI, 45.6% to 59.5%) in patients with unprovoked DVT and 22% in those with secondary DVT (95% CI, 17.2% to 27.8%).10 Other important risk factors to develop recurrent DVT are age older than 65 years, incomplete thrombus resolution, and iliofemoral thrombosis.6,9,11–13
Treatment Options
To improve the long-term natural history of DVT, it is important to preserve venous function and outflow. Overall, the first line of treatment for DVT remains anticoagulation using either low-weight-molecular heparin (LMWH) or unfractionated heparin (UFH). Nonetheless, a review of 13 studies of proximal DVT showed total and partial resolution in only 4% and 14% of patients, respectively, who were treated with anticoagulation.14
Venous thrombectomy was first attempted in extreme cases of extensive DVT with impending venous gangrene aiming for limb salvage.15,16 Indications for surgical thrombectomy are extensive proximal (iliofemoral) DVT when thrombolytic agents are contraindicated.17 Therefore surgical thrombectomy has still not gained popularity, being performed in only a few specialized centers.18 More recently, local thrombolysis and venous thrombectomy have been used together with very good outcomes.19 Conversely, development of dedicated devises and safer use of thrombolytic agents has expanded percutaneous procedures. The goal with thrombolysis is to provide early thrombus removal with a minimally invasive procedure and low complications. By restoring venous flow, the objective is to prevent valve damage, venous hypertension, and recurrent thrombosis in an attempt to prevent PTS.
Patient Selection
Recommendations and patient’s eligibility criteria for endovenous thrombectomy and thrombolysis via catheter-directed thrombolysis (CDT) or pharmacomechanical thrombectomy (PMT) have been defined as follows17,20:
Modalities of Thrombolysis and Thrombectomy
Systemic Thrombolysis
Over the past 50 years, variable outcomes were reported with systemic thrombolysis. Analysis of 13 contemporary studies including 591 patients found that the success rate of anticoagulation with heparin only showed total dissolution, partial lysis, and no improvement of the thrombus in 4%, 14%, and 82%, respectively.14 Improvement with systemic thrombolysis was found in 45% of the patients in the same review.
Advantages of systemic infusion of thrombolytic agents were faster resolution of the clot load and less venous valve dysfunction compared with anticoagulation alone.14 Nonetheless, the disadvantages of the technique include variable outcomes with potential serious complications such as increased risk of intracranial hemorrhage due to higher doses required to dissolve a distant thrombus.21 In light of the variable success rate, systemic complications, and current advances in minimally invasive endovenous techniques such as CDT and PMT, systemic thrombolysis has been abandoned and now belongs to historical reports.
Catheter-Directed Thrombolysis
The higher risk of bleeding complications of systemic thrombolysis secondary to administration of high doses of thrombolytic agents via peripheral veins led to studies on devices to deliver intrathrombus thrombolytic agents.21–23 In general, the technique consists of a multi–side-hole catheter that is positioned in the thrombus and remains parked in position to deliver localized thrombolytics and lysing the thrombus over time (Fig. 14-1).

Initial experience using CDT was reported by Semba and Dake using urokinase in 21 consecutive patients with iliofemoral DVT.24 Total thrombus lysis was achieved in 72% of the limbs with overall angioplasty or angioplasty with stents required in 64%.24 Subsequently, several series were published comparing anticoagulation alone with CDT.14,23,25 The impact on quality of life (QoL) in 68 patients who underwent CDT and 30 patients treated with anticoagulation alone was assessed by Comerota and colleagues.22 Notably, patients who underwent CDT reported better overall physical functioning, less stigma, and less health distress. Furthermore, health distress and symptoms were reduced in patients who had a successful versus a failed CDT treatment.
The caveats of initial studies related to a small number of patients and single-center observation were addressed by a multicenter registry study with urokinase in 473 patients that showed complete lysis of the thrombus in 31% and partial lysis in 52% of the limbs with better results in patients with acute symptoms of DVT.26 Patients with iliofemoral DVT had higher patency rates at 1-year follow-up than those patients treated for femoropopliteal DVT (64% versus 47%, p < .01), and the mean intensive care unit stay for monitoring thrombolytic therapy was 48 hours.26 One patient had fatal intracranial bleeding and another required surgical evacuation of a subdural hematoma.
Two prospective randomized clinical trials (RCTs) have been reported. The first RCT enrolled 35 patients comparing CDT with streptokinase versus anticoagulation alone; it showed 72% of the limbs in the CDT group with no obstruction or reflux versus only 12% in the anticoagulant group at 6-month follow-up.25 No major bleeding or mortality was reported. The second RCT, the CaVEnT (Catheter-directed Venous Thrombolysis) trial, enrolled 118 patients to assess the long-term functional efficacy with frequency of PTS after 24 months and descriptive efficacy at 6 months’ evaluation for patency rates.23 Patency of the iliofemoral vein segment was 64% in the CDT group and 36% in the control group. In addition, lysis greater than50% was achieved in 88% of the patients who underwent CDT.23
The long interval of CDT treatment course remains problematic because of institutional requirements of an intensive care unit setting for monitoring. A longer infusion interval that is needed also raises concern of potential risk of major bleeding found in up to 11% of the patients.26 In addition, the use of fluoroscopy for multiple follow-up venograms has directed efforts to accomplish thrombus removal in a more expeditious fashion than has currently been performed by PMT devices.17,27
Percutaneous Mechanical Thrombectomy
Two commercially available PMT devices are approved for treatment of DVT by the U.S. Food and Drug Administration (FDA): the Angiojet Thrombectomy system (Medrad/Possis Inc. Minneapolis, MN, and the Trellis-8 Peripheral Infusion System (Covidien, Mansfield, MA).28 In addition, a brief discussion about the Ekos Endowave system (Ekos Medical, Bothell, WA) is pertinent due to distinct mechanism combining ultrasound waves to facilitate chemical thrombolysis.
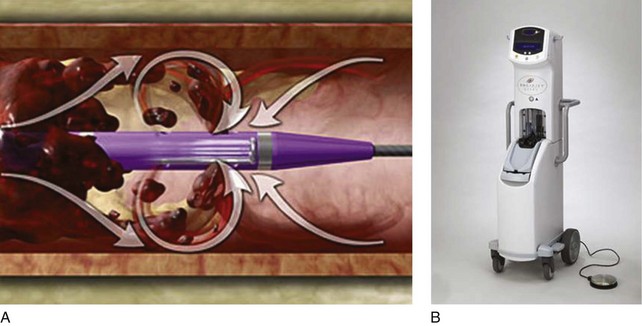
The mechanisms of PMT elicited by the Angiojet and Trellis device system are distinct. The Angiojet system is based on the Bernoulli-Venturi principle that states that high speed of a flow decreases the fluid pressure and creates a zone of vacuum (Fig. 14-2). Therefore the high-speed saline injections cause dissolution of the thrombus into small particles that are aspirated and eliminated through an effluent port. Theoretically, the advantages of the system are less endothelial damage and valve dysfunction. The device can also be used in combination with thrombolytics. Drug is delivered into the thrombus with the catheter, allowed to immerse in the thrombus, and then aspirated with the effluent port opened.
Initial experience was reported by Kasijaran et al. in 17 patients showing 59% of overall (>50%) thrombus removal.28 Bush et al. used the system in 23 limbs and reported complete and partial thrombus resolution in 65% and 35%, respectively.29 A comparison between the Angiojet versus CDT using only urokinase showed reduced treatment duration and lower costs with the Angiojet pulse system.30 Another study of 93 patients treated for symptomatic proximal DVT showed lower mean intensive care unit stays and overall length of hospital stays and lower total hospital costs with Angiojet compared with CDT only.27 One of the shortcomings of the system is a larger amount of fluid used to dissolve the thrombus, which can be impeditive in patients under fluid restriction, suggesting that precautions be used in cases of renal failure and decompensated congestive heart failure. Provoked hemolysis with increased bilirubin release in patients with liver failure may be another contraindication.
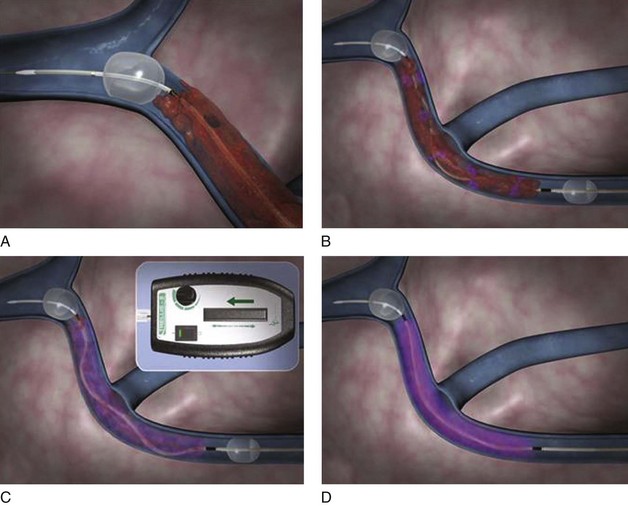
The Trellis-8 Peripheral Infusion System uses a dispersion spiral wire at higher spinning motion to macerated the thrombus in an isolated venous segment between a proximal and distal end balloon (Fig. 14-3). Initial experience with the device showed overall thrombus resolution in greater than 95% of limbs treated.31,32 No major complications including PE or major bleeding were reported. Trabal et al. reported a series of 25 limbs treated with the Trellis system showing greater than 50% thrombus resolution in 92% of the limbs with significant shorter treatment time and reduced thrombolytic agent used compared with CDT.33 In addition to thrombus burden resolution, the advantages of the Trellis system are its safety in patients with contraindications to thrombolytic agents and potentially less distal embolization due to isolation of a venous segment between two balloons.
The Ekos endowave functions by emitting high-frequency ultrasound waves that cause disaggregation of the fibrin in the thrombus, increasing permeability to the thrombolytic agents (Fig. 14-4).34 The catheter consists of four lumens from 6 to 50 cm of functional area containing an ultrasound wire and three other ports for thrombolytic agents and saline infusion. Initial experience in a study of 53 limbs with acute, chronic, and acute-on-chronic DVT showed complete thrombus removal in 70% and overall (complete and partial) lyses rate of 91%.35 There was no intracranial or retroperitoneal hematoma reported throughout the study. Further prospective, randomized studies on the use of the ultrasound-assisted thrombolysis are still expected.
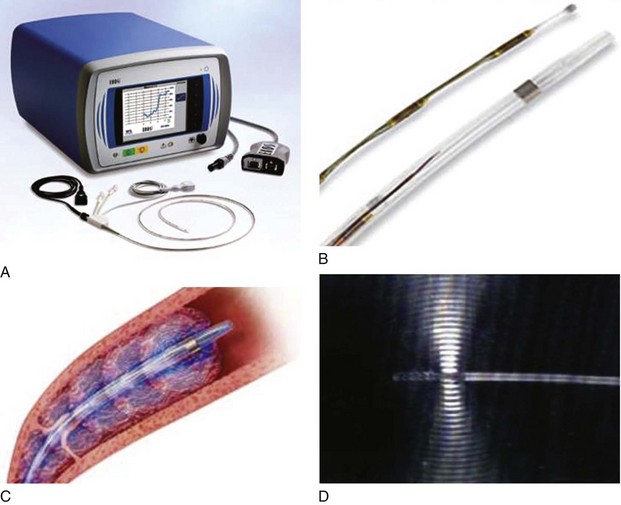
Fig 14–4 Ekos Endowave system. A, Ultrasound (US) source generator with monitor. B, Ultrasonic catheter
infusion. D, Detail of ultrasonic wave being emitted from distal probe.
An ongoing randomized multicenter trial, the ATTRACT trial, is designed to enroll 692 candidates to either PMT with anticoagulation versus anticoagulation alone in patients with symptomatic proximal DVT to assess the occurrence of PTS at 24-month follow-up.36 The impacts on QoL, safety, and cost analysis are expected to be addressed.
Endovascular Supplies
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


