Endovascular Treatment of Thoracoabdominal and Pararenal Aortic Aneurysms
Timothy Chuter
The minimally invasive aspects of the endovascular approach are particularly appealing in cases of pararenal and thoracoabdominal aneurysm (TAAA). The affected segment of aorta has multiple branches to organs, such as the liver, with a limited tolerance for ischemia. It also lies in a relatively inaccessible position, high in the abdominal cavity behind the pancreas. Consequently, open surgical repair of this area is a challenging operation with many potential sources of morbidity.
While the high retroperitoneal location of a TAAA is no impediment to endovascular stent graft insertion, which employs the distal arterial tree as a route to the aneurysm, the aortic branches are more of a problem. Unlike the branches of other aortic segments, such as the arch and bifurcation, the branches of the thoracoabdominal aorta are not readily accessible downstream, and branches of the stent graft cannot be inserted directly through the target arteries.
The first reported cases of endovascular thoracoabdominal aneurysm repair employed multibranched unibody stent grafts. This ingenious approach was based on a complex system of catheters to direct and control deployment of the self-expanding branches. The main complications were endoleak and embolism. The combination of a reinforced fenestration and a bridging stent graft has also been used successfully to treat a small number of pararenal and thoracoabdominal aneurysms. This modular approach has been successful in the short term, but there are concerns for the long-term stability of the intercomponent connection. Our technique addresses this concern by equipping the primary thoracoabdominal component with relatively long, axially directed cuffs.
We were able to make the thoracoabdominal component from Zenith components, but we lacked the means to make a bridging stent graft with the necessary flexibility and low profile for insertion into the visceral arteries. Nor could we hope that industry would develop special technology for such a limited market as this. We had to use stent grafts developed for other purposes and modify our technique accordingly. Indeed, the search for a suitable device has been the rate-limiting step in the development of our method of endovascular thoracoabdominal aneurysm repair.
Method
Stent Grafts
We assemble the stent graft in situ from three sets of components, or modules. The Zenith-based aortic components are categorized as thoracoabdominal or infrarenal, depending on their location. The thoracoabdominal component has one proximal orifice and multiple distal orifices, one for each visceral branch and one for the infrarenal aorta. The trunk and legs of the infrarenal aortic components are essentially the same as in a standard Zenith Trifab AAA system (Cook, Inc.). A small stent graft is used to extend each branch of the thoracoabdominal component into the visceral branches of the aorta; hence the term visceral extension.
The celiac and superior mesenteric branches of the thoracoabdominal component are cut from the same tube of fabric as the trunk. As a result, the segment below these branches is much narrower than the segment above, and there is space to work outside the stent graft, whatever the size of the aorta at that level. The trunk of the stent graft is oversized at least 4 mm relative to the supraceliac aorta. Visceral branch diameter and location vary according to the findings of pre-operative imaging. Nevertheless, thoracoabdominal components from different patients have been surprisingly alike, to the point where one could be substituted for another. Radioopaque markers on the trunk indicate axial orientation. Other markers at the outer ends of visceral cuffs guide the level of implantation, while markers around the inner ends guide catheterization. The thoracoabdominal component has a barbed uncovered proximal stent, like the standard Zenith abdominal aortic stent graft.
Stent-graft Delivery Systems
The infrarenal aortic components and the branch extensions have their own delivery systems. The delivery system for the thoracoabdominal component has the size (22 French) and proximal tip of the Zenith thoracic aortic device, and the shaft of the Zenith abdominal aortic device. Safety wires secure the proximal and distal ends of the stent graft to the central pusher of the delivery system.
Other Equipment
The route from the brachial artery into the branches of the thoracoabdominal aorta is long and tortuous. We use a range of coaxial catheters to protect the aortic arch, prevent coiling, selectively catheterize the target arteries, and guide branch extensions into place. All those listed are manufactured by Cook, Inc. (Bloomington, IN). The large diameter (10-12 French) sheaths extend from the brachial artery into the
proximal end of the thoracoabdominal component. The smaller sheaths and guiding catheters fit inside the larger ones. The smaller sheaths have a range of tip configurations to help support the path from the cuff of the thoracoabdominal component to the branch artery. The 7 French catheters fit inside the small sheath and the guiding catheters. They are used for selective visceral artery catheterization. Once in place, they also serve as dilators for the surrounding sheaths. Long, small caliber catheters in a variety of tip configurations add another option for selective catheterization.
proximal end of the thoracoabdominal component. The smaller sheaths and guiding catheters fit inside the larger ones. The smaller sheaths have a range of tip configurations to help support the path from the cuff of the thoracoabdominal component to the branch artery. The 7 French catheters fit inside the small sheath and the guiding catheters. They are used for selective visceral artery catheterization. Once in place, they also serve as dilators for the surrounding sheaths. Long, small caliber catheters in a variety of tip configurations add another option for selective catheterization.
We used to use off-the-shelf sheaths, but we now have a range of Flexor sheaths specially made for this application. The outer sheaths are all 60 cm in length, and the inner sheaths are all 80 cm in length. The choice of sheath diameter depends on the type of covered stent being used as a branch extension. The lowest profile is the medium-sized JoMed, which can pass through a 7 French sheath. The largest JoMed requires an 8 French sheath, while the Fluency requires a 10 French sheath. Each inner sheath determines the minimum diameter of the corresponding outer sheath. If we stick to kink-resistant Flexor sheaths, the 7 requires a 9, the 8 an 11, the 9 an 11, and the 10 a 12.
The guidewires are all 35/1,000″ caliber and all are exchange length (>200 cm). Hydrophilic wires are used for primary catheterization. They are exchanged for stiffer Rosen-tip wires.
All the important steps in the procedure are image-guided, and the advantages of high-quality imaging in an interventional suite probably outweigh the advantages of overhead lighting and sterility in an operating room. It is possible to implant a multibranched stent graft using a mobile C-arm, but it is wise to have another in reserve in case of overheating.
We currently prefer the balloon-expanded PTFE-covered JoStent as a visceral extension. The diameter depends on the size of the target artery. JoStents that are 58 mm long are delivered on 6 cm-long 5 French balloons.
Procedure
Our technique has evolved over the past 4 years to reflect the lessons of our experience with this approach (see below), but the basic elements remain the same. Sometimes it is easiest to insert the extensions before inserting the abdominal components, as depicted in Figures 15-1, 15-2, 15-3, 15-4, 15-5, 15-6, 15-7; sometimes the reverse is true, as described below.
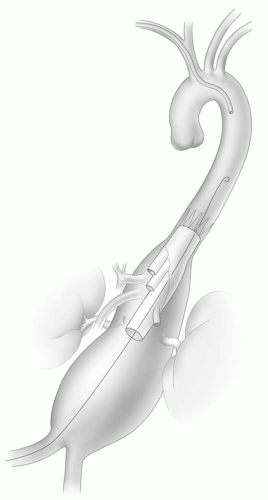 Figure 15-1. The primary thoracoabdominal component is inserted through the femoral arteries and positioned so that its branches lie just above the corresponding arterial orifices. |
Our technique is the following:
Expose and puncture both femoral arteries.
Give heparin (1 mg/kg), followed by additional doses to maintain an activated clotting time of approximately twice the baseline value.
Insert the thoracoabdominal stent-graft delivery system over a stiff wire (Lunderquist, Cook, Bloomington, IN) through one femoral artery, and an angiographic catheter through the other.
Perform aortograms to locate the celiac artery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


