Endovascular Revascularization for Extracranial Carotid Occlusive Disease
Endovascular Revascularization for Extracranial Carotid Occlusive Disease
Timothy M. Sullivan
Surgical endarterectomy of high-grade carotid lesions, both symptomatic and asymptomatic, has been identified as the treatment of choice for stroke prophylaxis in most patients when compared to best medical therapy (risk factor reduction and antiplatelet agents), as shown by the NASCET and ACAS studies. More careful inspection of their respective results suggests that the risk of disabling stroke or death was 1.9% in NASCET, with a 3.9% risk of minor stroke. In ACAS, the risk of major stroke or death was 0.6% when one excludes the 1.2% risk of stroke caused by diagnostic arteriography. Subsequently, carotid endarterectomy (CEA) has been performed in increasing numbers of patients, and it is now the most frequent surgical procedure performed by vascular surgeons. Despite the proven efficacy of CEA in the prevention of ischemic stroke, great interest has been generated in carotid angioplasty/ stenting (CAS) as an alternative to surgical therapy. This chapter will examine the indications, techniques, and results of this novel therapy.
While many studies, including ACAS and NASCET, have confirmed the safety and efficacy of CEA, there may in fact be categories of patients in whom CEA may not be optimal therapy. Hertzer et al. described the Cleveland Clinic experience for 2,228 consecutive CEA procedures in 2,046 patients from 1989 to 1995. The stroke and mortality rates for CEA as an isolated procedure were exemplary at 1.8% and 0.5%, respectively, for a combined rate of 2.3%. In addition, no statistical difference was found in stroke and mortality rates for asymptomatic patients, those presenting with hemispheric transient ischemic attack (TIA), or those operated for stroke with minimal residua. Those patients having combined CEA and coronary artery bypass grafting (CABG) had higher rates of peri-operative stroke (4.3%) and death (5.3%) than those patients having isolated CEA. Carotid reoperations were also associated with higher stroke (4.6%) and death rates (2%). These data lend credence to the idea that carotid endarterectomy can be performed safely in large groups of unselected patients, but they may give some insight into categories of patients who are at increased risk for operative intervention.
A follow-up study from the Cleveland Clinic by Ouriel and Hertzer et al. attempted to identify a subgroup of patients who, upon retrospective analysis, were at increased risk for CEA and therefore might be better served by CAS. From a prospective database over a 10-year period, 3,061 carotid endarterectomies were examined. A high-risk cohort (n = 594, 19.4%) was identified, based on the presence of severe (requiring angioplasty or bypass surgery within the 6 months prior to CEA) coronary artery disease (CAD), history of congestive heart failure (CHF), severe chronic obstructive pulmonary disease (COPD), or renal insufficiency (serum creatinine greater than 3 mg%). The rate of the composite endpoint of stroke/death/myocardial infarction (MI) was 3.8% for the entire group (stroke 2.1%, MI 1.2%, and death 1.1%). This composite endpoint occurred in 7.4% of those considered high risk (n = 594, 19.4%), significantly higher than in those 2,467 patients in the low-risk category (2.9%, p = 0.008). Patients in the high-risk group were further subdivided into those who had CEA alone and those in whom CEA was combined with CABG. Not surprisingly, the incidence of the composite endpoint was greater in those having combined CEA/CABG than those having CEA as an isolated procedure. In those having CEA alone, the risk of death was significantly greater in the high-risk group (p < 0.001). Importantly, however, while the risk of the combined endpoint stroke/death/MI was greater in the high-risk group, this difference did not reach statistical significance (p = 0.078). In addition, the rates of the individual endpoints of MI and stroke did not differ statistically between the high- and low-risk groups. These data from the Cleveland Clinic vascular surgery registry seem to support the notion that patients enrolled in the multicenter trials of CEA (NASCET and ACAS) were likely similar to the low-risk group, while those in the high-risk group may not in fact have had such stellar outcomes if included in multicenter trials. Other authors have called into question the very idea of “high-risk” CEA; conflicting data exist as to factors such as high lesions, reoperations, cervical radiation, and contralateral carotid occlusion. Subsequent trials have therefore focused on medically compromised, high-risk patients as those who may benefit from an alternative procedure such as CAS.
Carotid Angioplasty/Stenting
Indications
The basic indications for carotid angioplasty and stenting do not differ from those of standard surgical carotid endartectomy:
Table 28-1 Indications for CAS in High-Risk Patients
1.
Severe cardiac disease
A.
Requiring coronary PTA or CABG
B.
History of congestive heart failure
2.
Severe chronic obstructive pulmonary disease
A.
Requiring home oxygen
B.
FEV1 <20% predicted
3.
Severe chronic renal insufficiency
A.
Serum creatinine >3.0 mg%
B.
Currently on dialysis
4.
Prior carotid endarterectomy (restenosis)
A.
Contralateral vocal cord paralysis
5.
Surgically inaccessible lesions
A.
At or above the 2nd cervical vertebra
B.
Inferior to the clavicle
6.
Radiation-induced carotid stenosis
7.
Prior ipsilateral radical neck dissection
Asymptomatic lesions that fall within the 80% to 99% range on duplex ultrasound, which correlates with an angiographic stenosis of at least 60%. Most clinical trials of CAS in asymptomatic patients require an angiographic stenosis of at least 80% for study inclusion.
Symptomatic patients (hemispheric TIA, amaurosis fugax, or stroke with minimal residua) with at least a 70% angiographic stenosis. Patients with symptomatic, ulcerated stenoses greater than 50% may benefit from endarterectomy; this has not yet been extrapolated to carotid intervention. A list of the possible indications for CAS in high-risk patients and relative contraindications to the procedure are listed in Tables 28-1 and 28-2.
Table 28-2 Limitations of and Contraindications to CAS
Inability to obtain femoral artery access
Unfavorable aortic arch anatomy
Severe tortuosity of the common or internal carotid arteries
Table 28-3 Current Results of Carotid Angioplasty/Stenting
Author/Year
N (Arteries)
% Symptomatic
Cerebral Protection
Stroke + Death
Diethrich 1996
117
28%
No
7.3%
Yadav 1997
126
59%
No
7.9%
Henry 1998
174
35%
Mixed
2.9%
Bergeron 1999
99
44%
No
2%
Shawl 2000
192
61%
No
2.9%
Roubin 2001
604
52%
Mixed
7.4%
Ahmadi 2001
298
38%
Mixed
3.0%
CAVATAS 2001
251
96%
No
10%
Brooks 2001
53
100%
No
0%
d’Audiffret 2001
68
30%
Mixed
5.8%
Chakhtoura 2001
50
39%
No
2.2%
Baudier 2001
50
98%
Mixed
6%
Reimers 2001
88
36%
Yes
2.3%
Paniagua 2001
69
16%
No
5.6%
Criado 2002
135
40%
Mixed
2%
Guimaraens 2002
194
92%
Yes
2.6%
Al-Mubarak 2002
164
48%
Yes
2%
Bonaldi 2002
71
100%
Mixed
5.6%
Kao 2002
118
75%
No
4.2%
Whitlow 2002
75
56%
Yes
0%
Qureshi 2002
73
37%
Mixed
4.1%
Macdonald 2002
50
84%
Yes
6%
Stankovic 2002
102
37%
Mixed
0%
Kastrup 2003
100
63%
Mixed
5%
Cremonisi 2003
442
57%
Yes
1.1%
Terada 2003
87
80%
Yes
2.3%
Bowser 2003
52
60%
No
5.7%
Wholey 2003
12,392
53%
Mixed
4.75%
Becquemin 2003
114
33%
Mixed
7.0%
Dabrowski 2003
73
Not stated
Mixed
5.5%
Cernetti 2003
104
26%
Yes
4%
Bush 2003
51
29%
No
2%
Lal 2003
122
45%
Mixed
3.3%
Total 16,758
Weighted average
4.6%
Results of CAS Short-term Results
The short-term results of CAS mainly depend upon the presence or absence of cerebral embolization. With the addition of cerebral protection to the procedure, associated stroke risk seems to have decreased. Admittedly, however, improvements in devices and technology have created a moving target, making evaluation of results difficult at best. Nevertheless, a reasonable summary of the procedure, as it exists today, can be created from the available literature.
A list of studies is included in Table 28-3; only those that are peer-reviewed and that report on 50 or more patients are included.
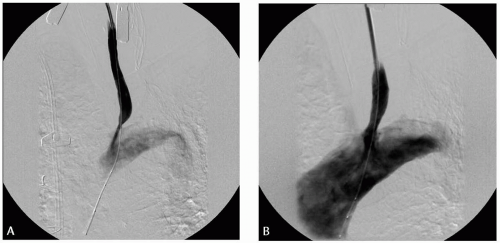
Proximal common carotid artery (CCA) lesions are relatively uncommon when compared with bifurcation lesions, but they may be well treated with angioplasty and stenting. In the author’s experience, most are treated via common carotid cutdown, retrograde angioplasty, and placement of a balloon-expandable stent, typically via a 7-French sheath (Fig. 28-1). Of 14 consecutive procedures performed at the Cleveland Clinic, one was converted to carotid-subclavian transposition following iatrogenic dissection, and two other procedures resulted in stroke secondary to internal carotid artery thrombosis. In both cases, which were performed in conjunction with redo bifurcation endarterectomies, the common carotid was patent at the time of surgical re-exploration and internal carotid thrombectomy. While the carotid stent procedure was not likely implicated, caution is urged when performing these combined procedures.
Restenosis
Table 28-4 lists restenosis rates following CAS. Again, only those peer-reviewed studies reporting more than 50 patients are included. While the rates of restenosis vary widely, most studies report 10% to 15% restenosis at 2 years following CAS.
Figure 28-1. A: High-grade stenosis of left common carotid artery (CCA), visualized via retrograde cutdown. B: Following angioplasty and primary stenting with a balloon-expandable stent.
Only gold members can continue reading. Log In or Register to continue