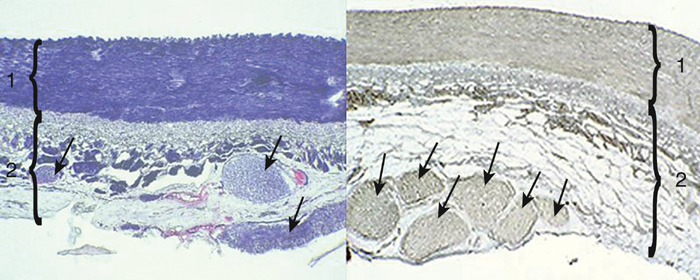
The renal sympathetic fibers travel in the adventitia of the renal artery, and all the current approaches to renal denervation involve nonselectively denervating the kidney by ablating the renal artery adventitia (Figure 1). The most commonly used approach involves radiofrequency (RF) ablation, although ultrasonic, laser, and chemical ablation have also been evaluated in human and animal studies. The currently used methods ablate both afferent and efferent fibers, and the clinical impact of the technique reflects the effect of total renal denervation.
Endovascular Renal Denervation
Resistant Hypertension and the Role of Sympathetic Nervous System
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


