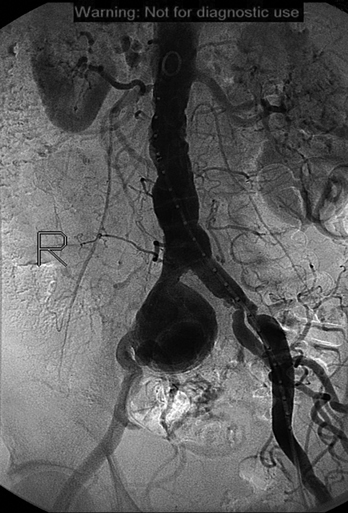
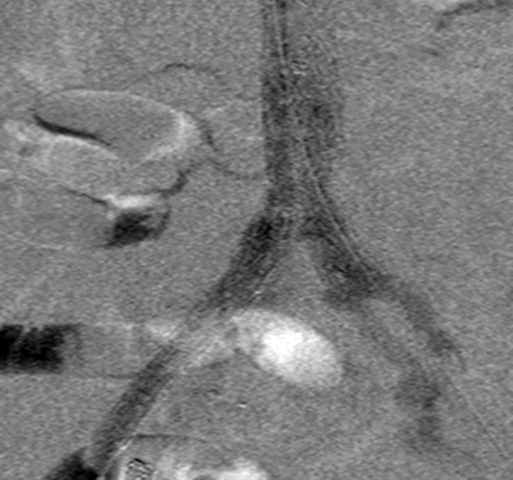
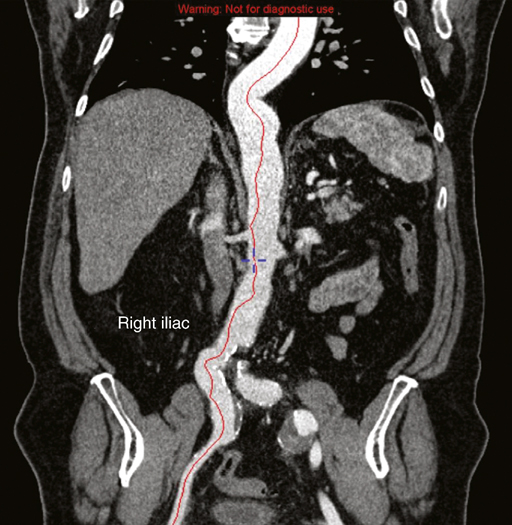
The endovascular management of IAAs requires meticulous preoperative imaging and planning. In general, this consists of a computed tomography angiogram (CTA) with fine cuts (2 mm). Multiplanar three-dimensional reconstructions can be used to delineate complex anatomy (Figure 1). This can be especially important in treating internal iliac artery aneurysms, which can have multiple outflow vessels that can require embolization. In addition, diagnostic angiography may be performed to obtain accurate measurements for graft sizing (Figure 2). Angiograms done with calibrated catheters can be very useful in determining the correct length of the device, especially in tortuous vessels. Often, adequate proximal and distal seal zones are not present, and adjunctive measures must be taken to repair the isolated IAA. For aneurysms involving the origin of the internal iliac artery, or for aneurysms without adequate length (15 mm) of normal vessel before the takeoff of the internal iliac artery, the origin of the internal iliac artery is embolized with coils or an endovascular plug (Figure 3). Embolization is performed to prevent perfusion of the iliac aneurysm from retrograde flow in the internal iliac artery once the stent graft has been deployed across its origin (type II endoleak). The stent graft is then placed across the origin, and the seal zone is created within the external iliac artery.
Endovascular Management of Isolated Iliac Artery Aneurysms
Preoperative Planning and Imaging
Operative Technique
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine