Chapter 10 Endocardial Fibroelastosis
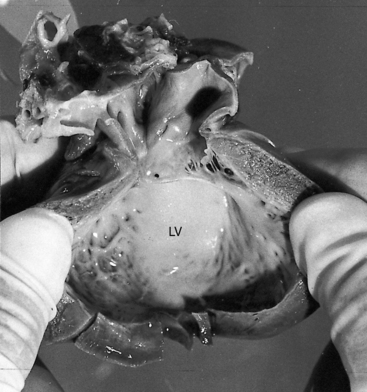
Endocardial fibroelastosis, a self-defining term introduced in 1943,1 is characterized by an opaque, pearly-white thickening that results from proliferation of collagen and elastic fibers (Figure 10-1).2,3 Isolated endocardial fibroelastosis involves the endocardium of a dilated hypertrophied left ventricle,2,3 hence the term primary endocardial fibroelastosis of the dilated type. Conversely, albeit rarely, the left ventricular cavity is small, hence the term endocardial fibroelastosis of the contracted type.2,3 Another form of endocardial fibroelastosis is considered secondary because it accompanies certain congenital malformations of the heart,3 especially aortic stenosis,4 coarctation of the aorta,5 anomalous origin of the left coronary artery from the pulmonary trunk,6 and hypoplastic left heart.7 Endocardial fibrosis is a substrate for mural thrombosis, which sets the stage for systemic emboli.8,9 The endocardium occasionally calcifies.
Pathogenesis takes into account the gross and histologic endocardial abnormalities and ventricular hypertrophy that characterize primary endocardial fibroelastosis of the dilated type. Fibroelastosis per se is a response to a variety of endocardial stimuli, with intrauterine endocardial injury as the common denominator.10–14 The disorder has been reported with or without complete heart block in fetuses and children of mothers who are positive for anti-Ro or anti-La antibodies.15,16 Fibroelastosis occurs in infants and adults after myocardial infarction,9,17 underscoring the endocardial response to injury.
Primary dilated endocardial fibroelastosis is the type that occurs in infants.18,19 Beyond infancy, the endocardial lesion tends to be patchy and is associated with myocardial fibrosis. The relationship between the infantile, the adolescent, and the adult form of the disease is unclear,18–21 and the relationship between the dilated and nondilated types has not been established.3,10,22
Primary endocardial fibroelastosis of the dilated type principally involves the left ventricle.3,23,24 The left atrium, right atrium, and right ventricle are only occasionally affected.25,26 Mitral regurgitation coexists with the dilated type3,27 because the papillary muscles originate high on the left ventricular wall (i.e., from the upper third) and accordingly exert undesirable lateral axes of tension on the chordae tendineae and mitral cusps, resulting in faulty leaflet apposition.3 In addition to being laterally aligned, the chordae tendineae are short and thick,26,27 and the papillary muscles tend to be small with histologic changes that resemble infarction.27
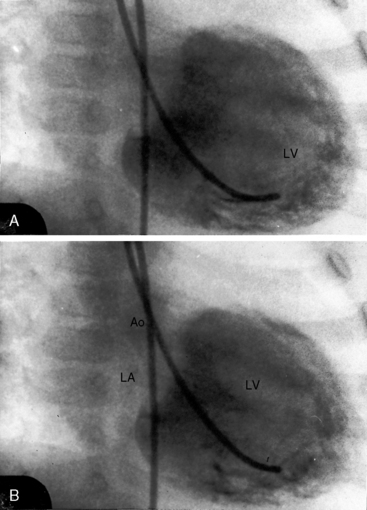
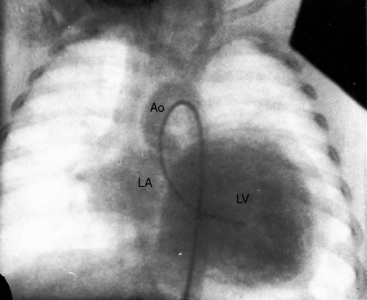
The physiologic consequences of primary endocardial fibroelastosis of the dilated type reflect the basic disorder of left ventricular endocardium, in concert with mitral regurgitation (Figures 10-2 and 10-3). Endocardial thickening restricts contraction of the dilated left ventricle and is responsible for global hypokinesis (see Figures 10-1 and 10-2).23 Elevated pressure in the left atrium, pulmonary veins, and pulmonary artery result in high left ventricular filling pressure and mitral regurgitation.23 Pulmonary hypertension is more pronounced in the nondilated form of the disease because the filling pressure in the small left ventricle is especially high.22,28
History
Primary endocardial fibroelastosis of the dilated type is equally distributed between the genders.29 It has been reported in siblings, in identical twins,30–32 and in more than one generation.20,33,34 The disease manifests itself in the first 6 to 12 months of life.3,29 Most affected children do not live beyond their second birthday.2 Prognosis is especially poor in neonates.14 Symptoms can run a protracted course and can begin suddenly, and death can be sudden and unexpected.2,35,36 Systemic emboli from left ventricular mural thrombi result in serious neurologic sequelae.2,8
Arterial pulse
The slow rate of rise is because of impaired left ventricular contractility. Sinus tachycardia and pulsus alternans are reflections of heart failure.2
Auscultation
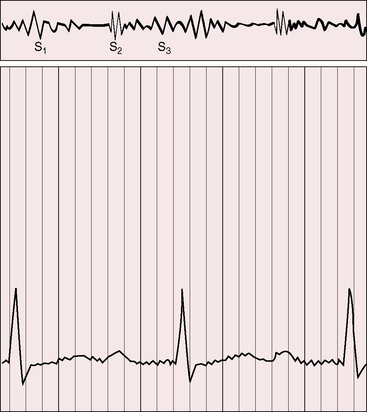
Hypokinetic left ventricular contraction diminishes the murmur of mitral incompetence despite appreciable regurgitant flow (Figure 10-4).2,29 Elevated pulmonary artery pressure augments the pulmonary component of the second heart sound and narrows the splitting. A third heart sound reflects the decrease in left ventricular distensibility2,23,29 and is especially prominent when mitral regurgitation coexists. Third and fourth heart sounds can summate to produce a triple rhythm or a short mid-diastolic murmur (see Figure 10-4).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


