The most striking feature of this electrocardiogram (ECG) is a markedly wide QRS complex with an S wave that merges with a peaked T wave without an isoelectric ST segment ( Figure 1 ). This is best seen in leads I and V 4 to V 6 . No definite P waves are seen, although a long PR interval and fusion of Ps with the preceding T waves cannot be excluded in leads II and V 2 . This is the ECG of severe hyperkalemia ; it belongs to a 35-year-old man with renal failure and a serum potassium level of 8.7 mEq/L.
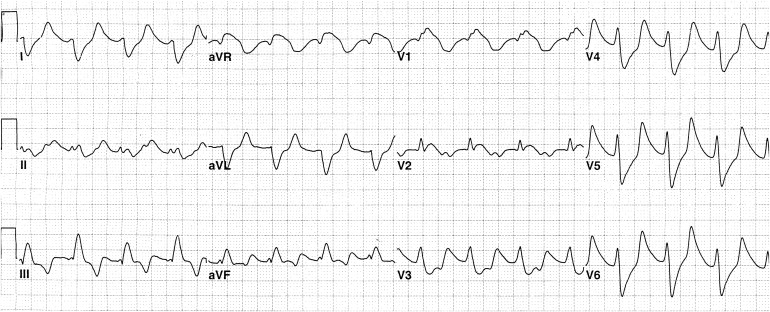
As the serum potassium level rises above the upper limit of normal (5.0 mEq/L), the first electrocardiographic change noted usually is a peaked symmetrical T wave with a narrow base. With ever higher levels of serum potassium, conduction slows resulting in a wide, low P wave, a long PR interval, and a wide QRS complex with slurring of the S wave into a rapidly ascending limb of the T wave. Eventually P waves disappear, and the QRS comes to resemble a sine wave. Death may result from asystole or ventricular fibrillation. Although the ECG of hyperkalemia may resemble right or left bundle branch block or myocardial infarction, it is usually the absence of typical features of those conditions in someone with the electrocardiographic features described previously and a reason for hyperkalemia that alert the physician to the correct diagnosis. The commonest cause of hyperkalemia is renal failure, and the patient’s ECG may also reflect hypocalcemia or left ventricular hypertrophy before the ECG is severely distorted as in this case.
Hyperkalemia can be rapidly fatal, especially when the ECG looks like the one shown here. Effective acute treatment methods include intravenous (IV) calcium gluconate, IV hypertonic glucose with insulin to facilitate themovement of glucose and potassium from the extracellular fluid into cells, and IV sodium bicarbonate. The sodium-cycle cation exchange resin polystyrene sulfonate given in 70% sorbitol as a retention enema is usually the next step and if necessary can be followed by oral doses. Prevention of recurrent hyperkalemia requires recognition and elimination of its causes. In this patient with chronic renal failure, a combination of the aforementioned measures followed by more frequent hemodialysis resulted in normokalemia.
Disclosures
The authors have no conflicts of interest to disclose.
See page 162 for disclosure information.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


