Growth differentiation factor-15 (GDF-15) is produced by cardiomyocytes and atherosclerotic lesions under stress conditions, but little is known about its relation with severity and complexity of coronary lesions. The aim of this study was to investigate the association between GDF-15 and the syntax score for risk prediction of major adverse cardiovascular events (MACE) at 2-year follow-up in patients with non–ST-segment elevation acute coronary syndrome (NSTEACS). This is a prospective cohort study of 502 patients with NSTEACS. The syntax score was calculated from baseline coronary angiography. Blood samples were obtained at study entry for the assessment of GDF-15 and high-sensitivity C reactive protein. One hundred and three patients (20.5%) showed MACE at 2-year follow-up. Patients who developed MACE had greater GDF-15 concentrations and syntax score (p <0.001) compared to patients who did not. There was a positive, but moderate, correlation between GDF-15 and syntax score (ρ = 0.45, p <0.0001). On Cox regression analysis, only GDF-15 levels (p <0.001), body mass index (p = 0.04), and syntax score (p <0.001) remained independent predictors of the MACE. The area under the curve of GDF-15 (0.912, 95% confidence interval 0.894 to 0.944) was significantly greater compared to high-sensitivity C reactive protein and syntax score. In conclusion, in patients with NSTEACS, levels of GDF-15 at admission were correlated with the syntax score and independently associated with an increased risk of MACE during 2-year follow-up.
The use of biomarkers as tools for prognosis assessment has demonstrated potential importance for identifying groups at greater risk who may benefit from more intensive prevention and treatment. Moreover, the burden of coronary atherosclerosis is closely associated with prognosis in coronary artery disease and the monocyte and/or macrophage activation plays a significant role in atherogenesis and plaque vulnerability and thus may determine rapid coronary artery disease progression. Growth differentiation factor 15 (GDF-15) is a discovered protein in the transforming growth factor β superfamily that is involved with inflammatory and apoptotic pathways. GDF-15 is a relatively new biomarker that is produced and secreted, among others, by cardiomyocytes and activated macrophages. Previous studies have found that elevated levels of GDF-15 predict major adverse cardiovascular events (MACE) in patients with coronary artery disease and correlate with disease severity in patients with heart failure. The syntax score has been shown to be associated with MACE in patients irrespective of disease severity in different clinical situations. Because it is well known that the monocyte or macrophage activation is closely associated with the pathogenesis of coronary atherosclerosis, we believe that it is of paramount importance to investigate the ability of SS and GDF-15 to predict the risk of future MACE. On this background, in the present study, we sought to investigate the association between GDF-15 and the syntax score for risk prediction of MACE at 2-year follow-up in patients with non–ST-segment elevation acute coronary syndrome (NSTEACS).
Methods
From June 2012 to April 2013, consecutive patients with NSTEACS were admitted to a tertiary care hospital. Initially, a total of 586 patients were initially screened for analysis. Patients were eligible for enrollment if they had NSTEACS and at least 1 stenosis >50%. Exclusion criteria were history of previous myocardial infarction, history of systemic inflammatory diseases, hepatic failure, malignant diseases, severe renal failure, and patients with history of coronary artery bypass grafting. Finally, 502 patients were included in the study. Patients were stratified by the presence of MACE at 2-year follow-up. The research protocol was approved by the ethics committee of our institution. All patients gave written informed consent. Clinical data, including age, gender, cardiovascular risk factors, medical therapy at discharge, coronary angiogram, and biochemical parameters, were collected.
The primary objective of this study was to investigate the association between GDF-15 and the syntax score for risk prediction of MACE at 2-year follow-up after discharge. MACE was defined as the combined result of cardiovascular death, nonfatal myocardial infarction, or readmission for unstable angina. Annual telephone interviews were conducted with participants or their proxy to inquire about interval hospitalizations or death. For any reported event, medical records and death certificates were obtained.
NSTEACS included unstable angina and non–ST-segment elevation myocardial infarction. Unstable angina was defined as the presence of typical chest pain at rest with an electrocardiographic documentation of ischemia, whereas non–ST-segment elevation myocardial infarction was defined as the presence of typical chest pain associated with an increase of troponin levels. Myocardial infarction was defined using standard diagnostic criteria. Death and cause of death were verified by death certificates and review of medical records. Significant coronary artery disease was defined as >50% stenosis in at least 1 coronary artery. Total syntax score for each patient was calculated by assessing the total points assigned to each individual lesion in coronary arteries >50% stenosis and >1.5-mm diameter. Two cardiologists, who were blinded to the study patient data, assessed the angiograms, and syntax score was measured accordingly.
In patients with NSTEACS who were treated with percutaneous coronary intervention (PCI), this was performed according to the standard of care. The choice of anticoagulant (unfractionated heparin, low-molecular-weight heparin, bivalirudin), use of glycoprotein IIb/IIIa inhibitors, and the type of stent was left to the operator’s discretion. All patients were treated with 300-mg aspirin at clinical presentation and 600-mg clopidogrel loading dose at the time of PCI. After PCI, patients were treated with aspirin 100 mg/day indefinitely, and clopidogrel 75 mg/day was recommended for 1 year.
Serial venous blood samples were obtained on admission from 8 a.m. to 3 p.m. to avoid the diurnal variation of inflammatory biomarkers. Serum samples were obtained by centrifugation, after the formation of the blood clot, and stored at −70°C for subsequent analyses. Serum GDF-15 concentrations were measured using a commercially, enzyme-linked immunosorbent assay (BioVendor GmbH, Heidelberg, Germany). The lowest detection limit of GFD-15 is 30.2 pg/ml. Co-efficients of variation were 4.3% and 7.8% for intra-assay and interassay variabilities, respectively. Serum high-sensitivity C-reactive protein (hsCRP) was measured, by an ultrasensitive, enzyme-linked, immunosorbent assay kit (DRG Instruments GmbH, Germany). The lowest detection limit of hsCRP was 0.010 mg/l. Co-efficients of variation were 5.12% and 11.6% for intra-assay and interassay variabilities, respectively. Troponin I was determined immune enzymatically, using a technique based on sandwich enzyme-linked immunosorbent assay (Boehringer Mannheim, Germany). Co-efficients of variation were 2.2% and 5.9% for intra-assay and interassay variabilities, respectively. Personnel, blinded to patient’s baseline characteristics and clinical outcomes, carried out all measurements.
Results for normally distributed continuous variables are expressed as the mean value + standard deviation, and continuous variables with nonnormal distribution are presented as median values (interquartile intervals). Analysis of normality of the continuous variables was performed with the Kolmogorov–Smirnov test. Logistic regression was used to assess the univariate associations between continuous baseline characteristics and the combined end point, and the chi-square testing was used for discrete variables. Spearman correlations were used to analyze the correlation between GDF-15 and syntax score. We assessed independent predictors of MACE using a Cox regression analysis. Cox regression analysis parameters were obtained with the likelihood ratio test. Backward stepwise selection was used in all multivariate models to derive the final model for which significance levels of 0.1 and 0.05 were chosen to exclude and include terms, respectively. GDF-15 was entered in the model dichotomized by the optimal cut-off point derived by the receiver operating characteristic (ROC) analysis with the Zweig and Campbell method. Variables included in multivariate analyses were age, gender, and also those that showed a correlation in univariate analysis that was significant at the 20% significance level (body mass index, use of clopidogrel and angiotensin-converting-enzyme inhibitors discharge, syntax score, hs-CRP, and GDF-15 levels). The proportional assumption was tested graphically (log–log graph) and by mean of Schöenfeld residuals test. Concordance Harrell C-statistic was calculated for the final model. To examine the additional contribution of GDF-15 on top of syntax score, we assessed the Harrell C and the Akaike information criterion on the Cox regression models with and without GDF-15. We additionally examined the ROC curve of GDF-15, syntax score, and hsCRP for the study end point. Differences were considered to be statistically significant if the null hypothesis could be rejected with 95% confidence. The SPSS 20.0 statistical software package (SPSS Inc., Chicago, Illinois) and STATA 14 (STATA Corp LP; College Station, Texas) were used for all calculations.
Results
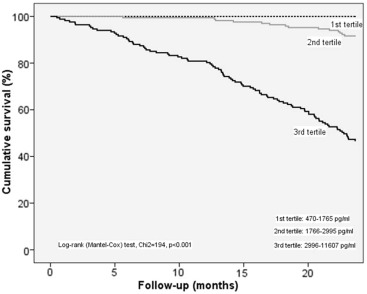
A total of 502 patients with NSTEACS were enrolled in the study. Table 1 lists baseline clinical characteristics. During 2-year follow-up, 103 patients (20.5%) experienced the study combined event, whereas 399 patients did not. Figure 1 shows the Kaplan–Meier survival curves for the combined end point by GDF-15 tertiles. Participants in the highest tertile had significantly higher rates of MACE compared with the lowest tertile. Clinical, angiographic, and biochemical characteristics of patients classified according to the presence or absence of events are provided in Table 2 . Univariate analysis showed that syntax score (p <0.001), hs-CRP serum concentration (p = 0.02), and GDF-15 serum concentration (p <0.001) were associated with the occurrence of the combined end point.
| Variables | (N = 502) |
|---|---|
| Age (years) | 64.8 ± 11.7 |
| Men | 400 (80 %) |
| Body max index (kg/m 2 ) | 27.5 ± 4.5 |
| Hypertension | 302 (60 %) |
| Smoker | 246 (49 %) |
| Dyslipidaemia | 283 (56 %) |
| Diabetes mellitus | 160 (32 %) |
| No of coronary arteries narrowed | |
| 1 | 246 (49 %) |
| 2 | 170 (34 %) |
| 3 | 86 (17 %) |
| Syntax Score | 20 [14-27] |
| Left ventricular ejection fraction (%) | 56.9 ± 9.6 |
| Hemoglobin (mg/dl) | 13.9 ± 5.9 |
| Hematocrit (%) | 40.1 ± 5.2 |
| Leukocytes (10 9 /l) | 10.0 ± 3.5 |
| Creatinine (mg/dl) | 0.9 ± 0.6 |
| Troponin I (ng/ml) | 33.2 ± 32.4 |
| Terapy of discharge | |
| Aspirin | 502 (100 %) |
| Clopidogrel | 439 (87 %) |
| Beta blockers | 446 (89 %) |
| Angiotensin-converting enzyme inhibitor | 354 (70%) |
| Statins | 502 (100 %) |
| Antidiabetic medication | 160 (32 %) |
| Variables | Events ( n =103) | No events ( n =399) | P |
|---|---|---|---|
| Age, years | 63.5 ± 11.6 | 65.1 ± 11.9 | 0.22 |
| Men | 82 (80 %) | 318 (80 %) | 0.9 |
| Body max index (kg/m 2 ) | 28.3 ± 4.8 | 27.4 ± 4.5 | 0.06 |
| Hypertension | 64 (62 %) | 238 (60 %) | 0.64 |
| Smoker | 45 (44 %) | 201 (50 %) | 0.22 |
| Dyslipidaemia | 59 (57 %) | 224 (56 %) | 0.83 |
| Diabetes mellitus | 38 (37 %) | 122 (31 %) | 0.22 |
| No of coronary arteries narrowed | |||
| 1 | 53 (51 %) | 193 (49 %) | 0.9 |
| 2 | 29 (28 %) | 141 (35 %) | |
| 3 | 21 (20 %) | 65 (16 %) | |
| Syntax Score | 27 [25-30] | 18 [14-23] | <0.001 |
| Left ventricular ejection fraction (%) | 57.2 ± 9.3 | 56.8 ± 9.8 | 0.7 |
| Hemoglobin (mg/dl) | 13.8 ± 1.8 | 13.9 ± 6.6 | 0.7 |
| Hematocrit (%) | 40.7 ± 5.1 | 40 ± 5.3 | 0.3 |
| Leukocytes (10 9 /l) | 10.3 ± 3.4 | 9.9 ± 3.6 | 0.4 |
| Creatinine (mg/dl) | 1 ± 0.7 | 0.9 ± 0.5 | 0.6 |
| Troponin I (ng/ml) | 34.7 ± 32.4 | 30.7 ± 32.9 | 0.3 |
| Total colesterol (mg/dl) | 167.5 ± 39 | 170.9 ± 45.7 | 0.4 |
| High-sensitivity C-reactive protein (mg/l) | 9.1 [5-21.6] | 7.4 [5-15.8] | 0.025 |
| Growth differentiation factor-15 (pg/ml) | 4862 [3545-6518] | 2027 [1404-2708] | <0.001 |
| Therapy at discharge | |||
| Aspirin | 103 (100 %) | 399 (100 %) | 1 |
| Clopidogrel | 85 (82 %) | 354 (89 %) | 0.09 |
| Beta blockers | 90 (87 %) | 356 (89 %) | 0.59 |
| Angiotensin-converting enzyme inhibitors | 78 (76 %) | 276 (69 %) | 0.19 |
| Statins | 103 (100 %) | 399 (100 %) | 1 |
| Antidiabetic medication | 38 (37 %) | 122 (31 %) | 0.22 |
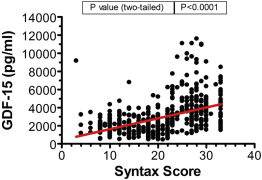
We also examined the correlation of GDF-15 with syntax score in patients with NSTEACS. As shown in Figure 2 , there was a positive, but moderate, correlation between GDF-15 and syntax score (Spearman correlation test, ρ = 0.45, p <0.0001). Figure 3 shows the proportion of patients with events classified according to values of median GDF-15 and syntax score. The primary outcome of cardiovascular death, nonfatal myocardial infarction, or readmission for unstable angina occurred in 54.9% (96 of 175) of patients with GDF-15 and syntax score above of median versus 6.6% (5 of 76) of patients with GDF-15 below of median.