Left transradial approach (TRA) for coronary angiography is associated with lower radiation parameters than right TRA in an all-comers population. The aim of this study was to determine the effects of left versus right TRA on radiation parameters in patients with predictors of TRA failure. Patients with predictors of TRA failure (≥3 of 4 following criteria: age ≥70 years, female gender, height ≤64 inches, and hypertension) referred to TRA operators were randomized to either right (n = 50) or left (n = 50) TRA, whereas those referred to transfemoral approach (TFA) operators were enrolled in a prospective registry (n = 50). The primary end point was the radiation measure of dose-area product (DAP). In an intention-to-treat analysis, DAP (34.1 Gy·cm 2 [24.9 to 45.6] vs 41.9 Gy·cm 2 [27.3 to 58.0], p = 0.08), fluoroscopy time (3.7 minutes [2.4 to 6.3] vs 5.6 minutes [3.1 to 8.7], p = 0.07), and operator radiation exposure (516 μR [275 to 967] vs 730 μR [503 to 1,165], p = 0.06) were not significantly different between left and right TRA, but total dose (411 mGy [310 to 592] vs 537 mGy [368 to 780], p = 0.03) was significantly lower with left versus right TRA. Radiation parameters were lowest in the TFA cohort (DAP 24.5 Gy·cm 2 [15.7 to 33.2], p <0.001; fluoroscopy time 2.3 minutes [1.5 to 3.7], p <0.001; operator radiation exposure 387 μR [264 to 557]; total dose 345 mGy [250 to 468], p = 0.001). Results were similar after adjustment for differences in baseline characteristics. In conclusion, median measurements of radiation were overall not significantly different between left versus right TRA in this select population of patients with predictors of TRA failure. All measurements of radiation were lowest in the TFA group.
There is a growing trend to perform invasive coronary angiography and percutaneous coronary interventions through transradial approach (TRA) versus transfemoral approach (TFA). Although this is partly due to patient preference and associated earlier ambulation times, recent large randomized trials demonstrate decreased rates of bleeding and access-site complications, as well as a reduction in major adverse cardiovascular events in the setting of acute coronary syndrome, with TRA versus TFA when performed by experienced operators. Left radial artery (LRA) access results in significantly lower parameters of radiation than right radial artery (RRA) access in an all-comers population, likely due to the associated lesser degree of subclavian artery tortuosity. However, the vast majority of TRA is performed through RRA due to greater ease for the operator. Certain patient characteristics are associated with TRA failure and include greater age, female gender, short stature, and a history of hypertension. It is uncertain whether LRA confers a similar advantage over RRA in this high-risk population. The aim of this study was to evaluate the effect of LRA versus RRA on parameters of radiation during invasive coronary angiography in patients with predictors of TRA failure. A secondary aim of this study was to compare radiation parameters associated with TRA versus TFA in this patient population.
Methods
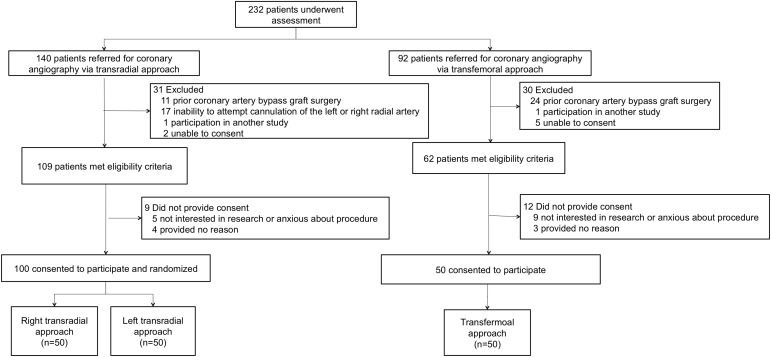
This study evaluated patients referred for coronary angiography from August 2012 to April 2015 at a single tertiary care center. Patients referred to TRA operators (n = 100) were randomized to LRA or RRA, whereas those referred to TFA operators were consecutively enrolled in a prospective single-arm cohort (n = 50). Eligibility criteria included the presence of ≥3 of the following 4 characteristics: age ≥70 years, female gender, ≤64 inches in height, and a history of treated hypertension. Exclusion criteria included (1) previous coronary artery bypass graft surgery, (2) inability to attempt cannulation of the LRA or RRA (e.g., abnormal Allen’s test, presence of arteriovenous fistula), (3) need for emergency cardiac catheterization, or (4) participation in another study ( Figure 1 ). Patients provided written informed consent, and the New York University School of Medicine Institutional Review Board approved the study. This investigator-initiated trial is registered at ClinicalTrials.gov (identifier: NCT01707524 ).
Operators in the present study either use a TRA (n = 5) or TFA (n = 3) as their primary approach due to experience in that respective approach, and the TRA operators have performed at least 100 procedures through the radial artery. Also in the present study although TRA operators are facile with both RRA and LRA, standard approach in the cardiac catheterization laboratory is RRA for comfort, with the exception of cases with a left internal mammary artery graft or a known reason for which RRA would be difficult (e.g., pulse not palpable or a history of right subclavian stenosis). However, for the purposes of this study, operators were agreeable to use either RRA or LRA. Coronary angiography was performed on an Artis Zee coronary angiography system equipped with software version VC14 and a ceiling mounted lead shield (Siemens AG, Germany). Access was obtained using either a 5- or 6- French hydrophilic sheath. The use of catheters, camera angles, and collimation was per operator preference. Pulsed fluoroscopy was used at a frame rate of 15 frames per second. Contrast was administered through an automated injector (Medrad, MEDRAD Inc., Pittsburgh, Pennsylvania). The use of a RadPad (Worldwide Innovations & Technologies Inc., Kansas City, Kansas) protective drape was encouraged when available.
Patient demographics were self-reported, and anthropometric data were measured by trained clinical nurses or study investigators. Pertinent medical history and the use of antihypertensive agents were obtained from review of the electronic medical system and confirmed by patient interview. Baseline laboratory data were performed in routine clinical laboratories within 30 days of the procedure. Procedural data were collected in real time.
The primary end point was dose-area product (DAP) measured in Gy cm 2 . Secondary end points included total radiation dose measured in mGy, fluoroscopy time measured in minutes, and operator radiation exposure measured in μR by a dosimeter placed in the left upper pocket of the lead apron worn by the primary operator. All parameters of radiation were recorded immediately after diagnostic coronary angiography was completed.
Sample size was calculated based on observational data of mean DAP 67.79 Gy·cm 2 during coronary angiography performed through RRA in our cardiac catheterization laboratory. We expected a 20% decrease with LRA in this study’s population. However, DAP is not normally distributed and, therefore, log-transformed DAP values were used for sample size calculation (mean 3.71 ± 0.34; estimated 5% decrease of log-transformed mean). Based on the previously mentioned assumptions, and a 2-sided 2-sample t test, the total sample size required to achieve 80% power at the 0.05 significance level was estimated to be 50 in each group.
Categorical variables are presented as proportions and compared between LRA and RRA groups using the Fisher’s exact or chi-square test, whereas continuous variables are presented as median (interquartile range) and compared between LRA and RRA groups using Mann–Whitney test. Comparisons across the LRA, RRA, and TFA groups were made using the chi-square test for proportions and Kruskal–Wallis test for continuous variables. Linear regression analysis was used to determine the effect of LRA versus RRA on radiation parameters after adjustment for baseline variables significantly different between LRA and RRA groups. Significance level was set at 0.05, and statistical analyses were performed on an intention-to-treat basis using Statistical Package for the Social Sciences 21.0 (IBM Corporation, Armonk, New York) and SAS 9.3 (SAS Institute Inc, Cary, North Carolina).
Results
Baseline demographic and clinical characteristics of the LRA, RRA, and TFA groups are listed in Table 1 . The proportion of patients with age ≥70 years was significantly lower, whereas the proportion of patients with height ≤64 inches was significantly higher, in the LRA versus RRA groups. There was no significant difference in proportion of female gender or history of hypertension, and the proportion of patients that met all 4 inclusion criteria did not significantly differ between LRA versus RRA groups (34% vs 48%, p = 0.22). Procedural characteristics of the LRA, RRA, and TFA groups are presented in Table 2 . In the LRA group, 2 subjects crossed over to RRA due to lack of arterial canalization, and 1 subject crossed over to TFA due to severe spasm of the radial artery. In the RRA group, 3 subjects crossed over to left TRA and 2 subjects crossed over to TFA due to lack of arterial canalization, whereas 1 subject crossed over to TFA due to a right subclavian occlusion diagnosed after arterial canalization.
| Variable | Left TRA (n = 50) | Right TRA (n = 50) | p- Value ∗ | TFA (n = 50) |
|---|---|---|---|---|
| Age (years) | 69 [62-75] | 75 [70-79] | 0.006 | 72 [65-78] |
| Age ≥70 years | 24 (48%) | 38 (76%) | 0.007 | 29 (58%) |
| Women | 47 (94%) | 44 (88%) | 0.49 | 44 (88%) |
| White non-hispanic | 8 (16%) | 6 (12%) | 0.83 | 22 (44%) |
| Black non-hispanic | 12 (24%) | 10 (20%) | 13 (26%) | |
| Hispanic | 20 (40%) | 21 (42%) | 8 (16%) | |
| Asian | 10 (20%) | 13 (26%) | 6 (12%) | |
| Height (cm) | 157 [152-160] | 157 [152-163] | 0.45 | 158[155-163] |
| Height ≤64 inches | 50 (100%) | 44 (88%) | 0.03 | 43 (86%) |
| Weight (kg) | 72 [63-81] | 71 [63-79] | 0.96 | 73 [62-81] |
| Body mass index (kg/m 2 ) | 29.5 [26.3-33.2] | 28.6 [26.7-32.2] | 0.86 | 29.8 [26.0-32.0] |
| Abdominal circumference (cm) | 107 [97-118] | 107 [99-115] | 0.87 | 104 [97-113] |
| Prior myocardial infarction | 5 (10%) | 6 (12%) | 1.0 | 3 (6%) |
| Prior percutaneous coronary intervention | 9 (18%) | 9 (18%) | 1.0 | 10 (20%) |
| Hypertension † | 45 (90%) | 47 (94%) | 0.72 | 48 (96%) |
| Hypercholesterolemia ‡ | 26 (52%) | 27 (54%) | 1.0 | 34 (68%) |
| Diabetes mellitus | 20 (40%) | 27 (54%) | 0.23 | 15 (30%) |
| Peripheral artery disease | 3 (6%) | 6 (12%) | 0.49 | 1 (2%) |
| Creatinine (mg/dL) | 0.8 [0.7-1.0] | 0.8 [0.7-1.0] | 0.75 | 1.0 [0.8-1.1] |
| Normal left ventricular ejection fraction | 46 (94%) | 45 (90%) | 0.43 | 42 (84%) |
∗ Comparison of right versus left TRA.
† Hypertension was defined as a clinical diagnosis of hypertension and on antihypertensive medications.
‡ Hyperlipidemia was defined as a clinical diagnosis of hyperlipidemia and on lipid-lowering agents.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


