6 Echocardiography
Imaging Methods and Clinical Applications
Transthoracic Echocardiography
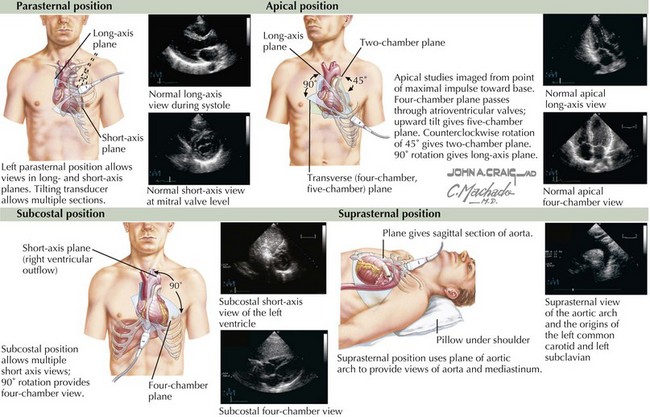
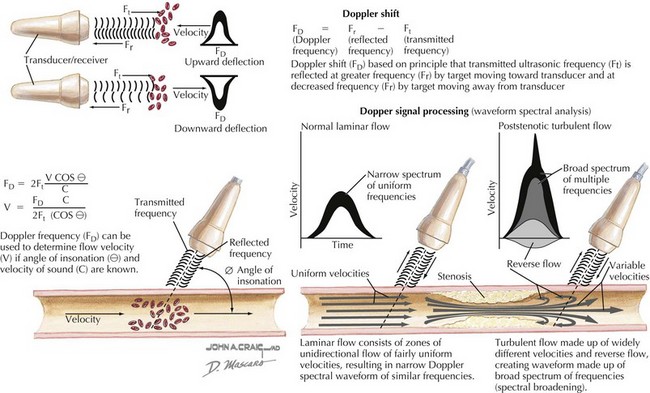
Transthoracic 2D echocardiography is the foundation of the clinical echocardiographic examination. Tomographic images from multiple locations on the chest wall, defined by the transducer position and image plane (Fig. 6-1), provide a reliable, portable, and reproducible evaluation of cardiac chamber sizes, myocardial thickness, ventricular contractile performance, valvular structure and function, the pericardium, and great vessels. Doppler echocardiographic assessment of the direction and velocity of blood flow within the heart and great vessels is valuable in the detection and quantification of obstructive lesions and valvular regurgitation (Fig. 6-2). Transthoracic 2D directed M-mode echocardiography is especially valuable in the evaluation of mitral and aortic valve motion in dynamic and fixed left ventricular outflow obstruction, in the timing of mitral valve closure in aortic regurgitation, and in the assessment of pericardial disease. This technique also provides a precise measurement of cardiac chamber sizes and wall thickness throughout the cardiac cycle allowing accurate estimates of overall left ventricular contractile performance and ejection fraction, provided there are no segmental wall motion abnormalities.