Echinococcal Disease
Presentation
A 46-year-old man with no significant past medical history presents to your office complaining of a nonproductive cough accompanied by dull pain in the right chest for the past 2 weeks. The patient is a sheep farmer on a trip from New Zealand who is visiting friends in your area.
On examination, he is noted to be febrile (temperature of 100.8°F), and the lungs are clear to auscultation.
▪ Chest X-rays
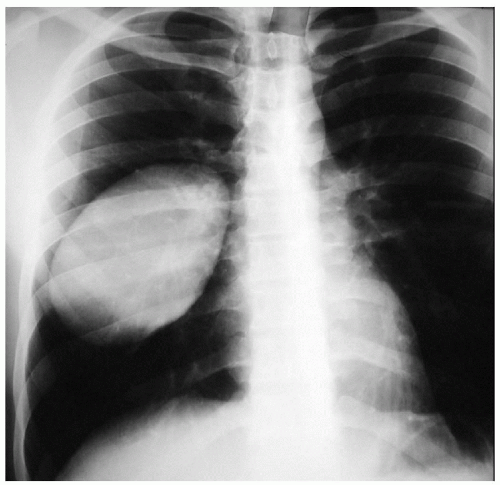 Figure 4-1 |
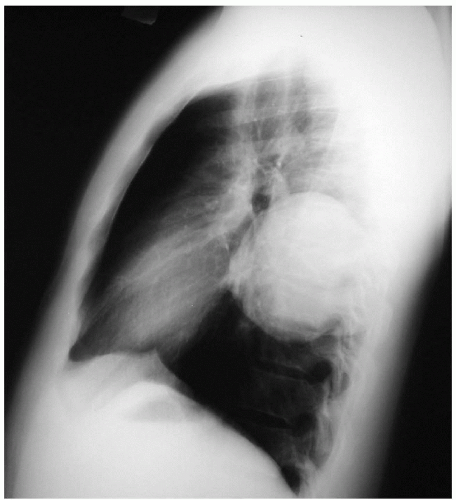 Figure 4-2 |
Chest X-ray Report
There is a smooth, dense, spherical opacity in the right lower lobe and no effusions. The heart is of normal size.
Differential Diagnosis
The differential diagnosis for chest masses of this type includes malignancy and infectious etiologies. In a patient from an endemic area, dry cough, fever, and pain with a smooth, round lesion are associated with echinococcosis. Endemic areas other then New Zealand include South Africa, Australia, South America, and Mediterranean countries.
Several radiographic signs that can further suggest the diagnosis include the following:
Escudero-Nenerow sign: a spherical to oval shape change observed with deep inspiration
Notch sign: an indentation in the bronchus from a centrally located cyst
Moon, crescent, or pulmonary meniscus sign: a crescent-shaped shadow from air between layers of the cyst indicating impending rupture
Double-domed arch sign: a result of air entering the cyst after rupture
Water lily sign: a result of an air and fluid layer produced by the floating membrane of the cyst
If the echinococcal cyst ruptures, a loculated hydropneumothorax may be present.
Discussion
Hydatid disease, caused by the Echinococcus granulosus tapeworm, is often found in cattle- and sheep-raising regions of the world. It should therefore be considered in a patient presenting with a well-defined round pulmonary density who has spent time in an endemic area. The organism is usually found in dogs, coyotes, and wolves that ingest echinococcal cysts from the intestines of their prey. The ova from the cysts are released in the feces, thereby contaminating water and vegetation.
In humans, once ingested, the parasite typically penetrates the small bowel mucosa, entering the portal system. However, entry by way of intestinal lymphatics or direct inhalation has also been suggested. The most common site of lodgment is the liver. The lung may be involved in 10% to 30% of cases and is usually accompanied by synchronous hepatic lesions. As the cysts rupture, ova enter the venous circulation and can result in secondary cyst formation.
Pulmonary echinococcosis usually affects the lower lobes and is more common on the right side. Cysts are multiple in 30% of cases and bilateral in 20% of cases and may develop more quickly and extensively in children.
Two types of cysts exist: unilocular and alveolar. The unilocular type is found in the lung. These cysts are thick walled and are filled with clear hydatid fluid. The wall has three layers: a germinal layer and laminated membrane from the parasite, surrounded by a pericystic zone or adventitia from the host. The inner germinal layer is a thin, transparent layer lined with capsules containing larvae, which can form daughter cysts suspended in the fluid. The laminated membrane is 1 to 3 mm in thickness and forms the plane for surgical dissection. The outer pericystic layer is formed by local reaction against the parasite, with infiltration by leukocytes and fibro blasts. Hepatic cysts usually calcify, although this is rarely seen in pulmonary cysts.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


