Chapter 18 EBUS-TBNA for Subcentimeter PET-Negative Subcarinal LAD (Station 7) and a Right Lower Lobe Pulmonary Nodule

Case Description
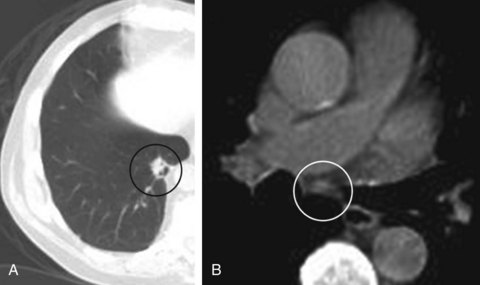
An 81-year-old man was referred for a 1.5 cm solitary pulmonary nodule in the medio-basal segment of the RLL, incidentally noted while he was undergoing CT of the abdomen for nephrolithiasis. An integrated emission tomography with CT/18F-fluoro-2-deoxy-d-glucose PET scan confirmed the nodule, showing a 5.5 SUV max on PET, and revealed a PET-negative 7 mm subcarinal lymph node (Figure 18-1). Vital signs and physical examination were unremarkable. Complete blood count, coagulation, chemistry panel, and spirometry and DLCO were normal. A treadmill stress test performed 6 months earlier was normal. PPD was negative, and the patient had no known exposure to tuberculosis. He smoked 1 pack/day for 25 years but quit 20 years before the time of his presentation. He was still working and active, playing golf 3 times a week. He lived with his wife, who was very involved in his care. He desired all available treatment options in case this was lung cancer.
Case Resolution
Initial Evaluations
Physical Examination, Complementary Tests, and Functional Status Assessment
Assessment of this patient’s functional status at the initial visit could guide additional diagnostic and therapeutic interventions. His age, smoking history, and imaging studies increased the likelihood that he had primary lung carcinoma. Treatment of lung cancer, whether with surgery, chemotherapy, radiation therapy, or a combination of these, can be associated with substantial toxicity. Patients with significant functional impairment due to their lung cancer or to comorbid conditions may not be able to withstand resection or, alternatively, aggressive chemoradiotherapy. The Karnofsky Performance Status (KPS) is a general measure of functional impairment that is used to compare the effectiveness of various therapies and to assess prognosis in individual patients: The lower the score, the worse the survival for most serious illnesses.1 The Eastern Cooperative Oncology Group (ECOG) Performance Scale uses a five-point scale and has been shown to be a better predictor of prognosis than KPS.2,3 Relevant to this case suspicious of smoking-related malignancy is that if diagnosis performed is locally advanced cancer (stage IIIA) based on his pulmonary nodule and the subcentimeter subcarinal lymph node (LN), this patient’s operability or eligibility for chemoradiotherapy could be precluded by poor performance status. However, his performance status was excellent, with KPS of 100 and ECOG score of 0.
Computed tomography (CT) scan showed a 1.5 cm right lower lobe (RLL) nodule and a 0.7 cm subcarinal LN. Although CT is accurate in detecting LN enlargement, the clinical relevance of LN enlargement for staging is poor, because large nodes may be benign and small nodes contain metastases in approximately 20% of cases.4 Of importance to this patient, 5.6% of patients with radiographic stage I disease in one study were eventually found to have N2 disease.5 Multiple studies and meta-analyses have demonstrated that noninvasive staging of lung cancer is improved by the use of positron emission tomography (PET) scanning.6 Owing to a high negative predictive value (NPV) of PET scanning of approximately 90%, invasive staging procedures are generally omitted in patients with clinical stage I non–small cell lung cancer (NSCLC) and negative mediastinal PET images. This strategy warrants caution, however, in the following situations, which increase the risk for occult N2 disease: larger tumor size (≥6.0 cm)—57% prevalence; central location—21.6% prevalence; high standardized uptake value (SUV) in the primary tumor (≥4.0)—10.5% prevalence; and adenocarcinoma cell type—9.0% prevalence.7 In these instances, PET results do not provide acceptable accuracy rates for mediastinal staging. Therefore invasive staging is usually advocated for patients with one or more risk factors for occult N2 disease.5,7,8 Routine use of invasive lymph node staging for patients with clinical stage I NSCLC and no risk factors for occult N2 disease, however, is neither necessary nor considered to be cost-effective.5 In our patient with a maximal standardized uptake value (SUV max) greater than 4.0 in the nodule, small but measurable LN (<10 mm), and suspected NSCLC, mediastinal staging was considered necessary.
Procedural Strategies
Indications
The status of the mediastinum is a most crucial factor in selection of an optimal treatment strategy for NSCLC; invasive confirmation of the radiographic stage is recommended, regardless of results of PET scan findings for mediastinal nodes.9 If our patient’s nodal station 7 is positive for malignancy, his clinical stage is IIIA-N2. Sampling station 7 in our patient is essential because the incidence of occult N2* disease in NSCLC patients with negative mediastinal uptake of 18F-fluoro-2-deoxy-d-glucose (18FDG) on PET-CT is reportedly around 16% (25 of 153 patients). The highest incidence of occult N2 involvement is seen in fact in station 7 (subcarinal) (16 of 25 patients; 64%) followed by station 4 (lower paratracheal) (7 of 25 patients; 28%).10 Flexible bronchoscopy in this patient would allow complete airway inspection to ascertain the absence of endobronchial lesions that could potentially alter staging and management,11 and to sample LN 7 at the same setting. Although nodal sampling could be done with the use of conventional TBNA, EBUS-TBNA might increase diagnostic yield, even at level 7, because of small lymph node size.12,13
Contraindications
No absolute contraindications to bronchoscopy with EBUS-TBNA were identified. We usually perform this procedure with the patient under general anesthesia; however, in our elderly patient, this approach could result in a number of physiologic changes that affect respiratory and cardiovascular function and may complicate the procedure.14 These age-related changes include lung parenchymal changes resulting in impaired gas exchange and reduced partial pressure of oxygen in arterial blood (PaO2); decreased lung elasticity and increased ventilation-perfusion mismatch; decreased chest wall compliance and respiratory muscle strength, leading to increased work of breathing and higher risk of respiratory failure; reduced cough and mucociliary clearance, and possibly neuromuscular deconditioning, increasing the risk for aspiration; and reduced responsiveness of brain respiratory centers to hypoxemia and hypercarbia and diminished overall cardiopulmonary reserve, resulting in heightened sensitivity to the negative inotropy and vasodilatory effects of induction agents and other vasoactive drugs. These concerns must be addressed with the anesthesiologist before the procedure is begun.
Expected Results
After complete airway examination has been performed with white light bronchoscopy, a complete sonographic mediastinal and hilar nodal assessment would be completed because of potential upstaging to N3 disease (stage IIIB),15 in case EBUS identified contralateral LNs positive for malignancy (microscopic N3 disease, which could render the patient unresectable). If complete EBUS mediastinal and hilar evaluation reveals no other nodes, then CT documenting LN 7 only would be sampled. EBUS-TBNA can reliably sample enlarged mediastinal LNs in patients with NSCLC, but most studies have addressed nodes visible on CT (>1 cm) or PET (SUV max >2.5). However, in one study, 100 patients highly suspicious for NSCLC on CT scans showing no enlarged lymph nodes (no node >1 cm) and a negative PET of the mediastinum underwent EBUS-TBNA. Identifiable LNs at locations 2R, 2 L, 4R, 4 L, 7, 10R, 10 L, 11R, and 11 L were aspirated, and all patients underwent subsequent surgical staging; diagnoses based on aspiration results were compared with those based on surgical results. The sensitivity of EBUS-TBNA for detecting malignancy was 89%, the specificity was 100%, and the NPV was 98.9%. Overall, 17 of 97 patients had stage N2 or N3 disease, of whom 16 were identified from EBUS-TBNA, and 4 had stage N1 disease, of whom 3 were identified by EBUS-TBNA. Investigators concluded that EBUS-TBNA could accurately sample and stage patients with clinical stage I lung cancer without evidence of mediastinal involvement on CT and PET. Based on these data, open surgical exploration could be avoided in 1 of 6 patients without CT evidence of mediastinal disease. If nonmalignant results are obtained from EBUS-TBNA, however, this should be followed by mediastinoscopy. Because potentially operable patients with no signs of mediastinal involvement may benefit from presurgical staging by EBUS-TBNA, even when LNs are small,16 we decided to proceed with EBUS-TBNA under general anesthesia.*
Team Experience
The team should be familiar with techniques and equipment because of the particularities of TBNA, EBUS, and EBUS-TBNA.17 Experience with sampling this station is high because LN 7 and right lower paratracheal nodes (station 4R) are the most commonly sampled nodes during conventional TBNA and EBUS-TBNA.12,13 At the time of this writing, American College of Chest Physicians (ACCP) guidelines for interventional pulmonary procedures state that trainees should be supervised for 50 EBUS procedures, and that a chest physician should perform 5 to 10 procedures per year to maintain competency.18 The European Respiratory Society/American Thoracic Society joint statement on interventional pulmonology recommends that initial training should consist of 40 supervised procedures, and 25 procedures should be done per year to maintain competency.19 The chest physician learning EBUS probably should be well acquainted with needle aspiration principles and should be trained to interpret endobronchial ultrasound images.20
Risk-Benefit Analysis
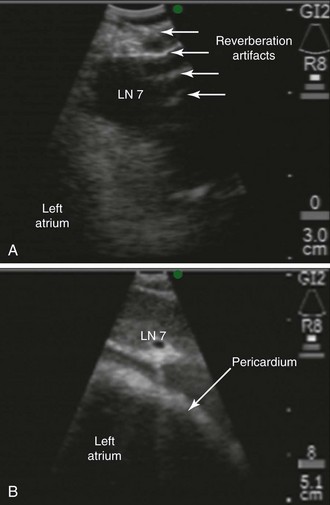
Although EBUS-TBNA has a high diagnostic yield and is safe, clinically significant and rare complications include pericarditis and pneumothorax requiring chest tube drainage.21 The risk of pericarditis is particular to this station because the subcarinal node could be adjacent to the pericardium (Figure 18-2); with the needle at its full extension (i.e., 4 cm), the operator may inadvertently penetrate the pericardium during EBUS-TBNA at this station. A false-negative result may be considered a “complication” because it could lead to death if inappropriate decisions are made (e.g., pulmonary resection in case of unrecognized N3, absence of indicated induction therapy in case of missed N2 disease).22 Thus the complication rate of EBUS-TBNA is higher than that of mediastinoscopy (24% false-negative rate for EBUS as compared with 10% for mediastinoscopy).9 We considered that the benefits of making a diagnosis and staging this patient outweighed the minimal associated risks.
Diagnostic Alternatives
For Diagnosis and Staging of the Mediastinum
1. Conventional TBNA: In one study, the yield of conventional TBNA for station 7 was 74% compared with 86% in the EBUS-guided group (difference not statistically significant).23 Other studies have shown higher diagnostic yields of 96% with EBUS for station 7.12
2. EUS-FNA has been used successfully for sampling station 7 and reportedly has a diagnostic yield similar to that of EBUS-TBNA.24 Although this technique is suitable for assessing LNs in the posterior part of levels 4 L, 5, and 7, and in the inferior mediastinum at levels 8 and 9, EUS alone has limited value for complete staging because right-sided LNs usually are inaccessible. Therefore EUS was not offered in this case.
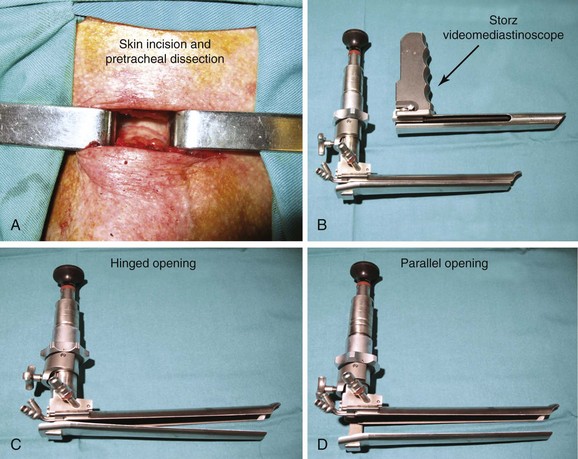
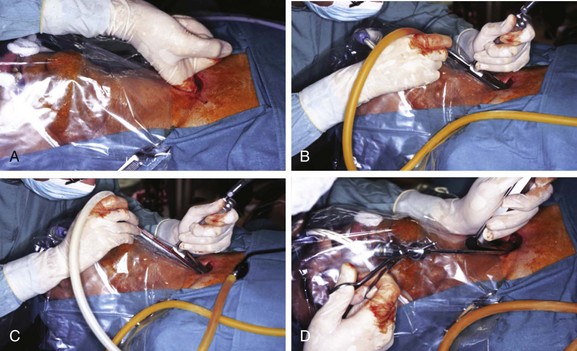
3. Mediastinoscopy: This open surgical biopsy technique is performed with the patient under general anesthesia. It could be recommended in this patient if endoscopic sampling of station 7 is negative for malignancy or is otherwise nondiagnostic.12 Rates of morbidity and mortality are low (2% and 0.08%, respectively).9 The average sensitivity of mediastinoscopy in detecting mediastinal node involvement from cancer is approximately 80%, and the average false-negative (FN) rate is approximately 10%9; half (range, 42% to 57%) of FN cases were due to nodes that were not accessible by the mediastinoscope. Sampling of station 7 is usually straightforward. The procedure involves an incision just above the suprasternal notch (Figure 18-3), insertion of a mediastinoscope alongside the trachea (Figure 18-4) and, ideally, systematic exploration and biopsy under visual guidance of at least one node from up to five nodal stations (2R, 4R, 7, 4 L, and 2 L), unless none are present after dissection in the nodal region. It is recommended to always biopsy the right and left lower paratracheal and subcarinal nodes. In this case, after risks and benefits were discussed, our patient preferred that we proceed with an endoscopic needle aspiration technique.
4. Video-assisted thoracic surgery (VATS): This procedure is usually reserved for subaortic (station 5) and anterior mediastinal (station 6) nodes. It can also be used for LN levels that are not accessible by routine mediastinoscopy (stations 8 and 9), in case these LN stations cannot be accessed by EUS-FNA, or when EUS-FNA specimens are nondiagnostic. The procedure is limited to assessment of only one side of the mediastinum (i.e., the side of the thoracoscopy). Sensitivity varies from 37% to 100%. Even in studies restricted to patients with enlarged nodes, sensitivity ranges from 50% to 100%. No mortality is reported from VATS for mediastinal staging, and complications are few, occurring in only 12 of 669 patients (average, 2%; range, 0 to 9%).9 VATS can also be used to further evaluate T stage, especially for detecting or excluding T4 lesions that preclude resection. True disease has been shown to be absent in 38% of patients (range, 29% to 50%) with radiographically suspected T4 involvement. Our patient did not have a separate tumor nodule in an ipsilateral lobe, and the primary tumor was not adjacent to the heart, trachea, carina, recurrent laryngeal nerve, or esophagus; however, it was relatively close to the aorta and the vertebral body (see Figure 18-1).
5. Combined EUS and EBUS: This should enable a complete evaluation of the mediastinum because of the complementary reach of each technique. Hwangbo et al.25 and Herth et al.26 reported on complete endosonographic staging of NSCLC using just a single EBUS scope to perform both EBUS and EUS. EUS-FNA using the same EBUS scope could be used as an add-on to EBUS only for those patients in whom nodes were inaccessible or difficult to reach by EBUS. As expected, this approach proved useful for sampling left lower paratracheal nodes (4 L), the aortopulmonary window (station 5), and the lower mediastinum (stations 8 and 9) but not for sampling station 7.
For Diagnosing the Pulmonary Nodule
An alternative approach in this case is to proceed directly with diagnosing the pulmonary nodule rather than sampling the PET-negative subcentimeter LN 7. In fact, a bayesian model suggests that the post-test probability of malignant involvement is very low (6%) if the mediastinum is normal on both CT and PET.27 One meta-analysis found a similar post-test probability for N2 disease of 5% for LNs smaller than 15 mm in the short axis on CT in patients with a negative PET result. Some experts suggest that patients in this group should be referred for thoracotomy and complete lymph node dissection, without prior mediastinoscopy.28 This approach could be justifiable in our patient with a high pretest probability for malignancy, and one could argue that even biopsying the pulmonary nodule may not be necessary before surgery because the risk for malignancy is high, given the patient’s history. Moreover, diagnostic bronchoscopic modalities have poor NPV for pulmonary nodules, prompting some authorities to advise against their routine use in patients with a high clinical likelihood of early-stage and surgically resectable lung cancer. In such cases, a negative result would still require surgical resection. Surgical removal of ultimately benign nodules has been reported in 20% and 49% of cases, meaning that many patients with benign nodules have been unnecessarily subjected to surgical resection.29
1. CT-guided transthoracic needle aspiration (TTNA): This technique has a high yield and low cost for pulmonary nodule diagnosis but is associated with frequent occurrence of pneumothorax (20% to 50%), with approximately 7% of patients requiring chest tube drainage.30 Certain lesions, such as the one seen in our patient, are difficult to access or increase risk for pneumothorax because of their small size or their location, or because of surrounding emphysematous lung parenchyma.31 Distance from the pleura affects diagnostic accuracy, which drops to 60% or less when the needle path length exceeds 40 mm.32
2. Standard white light bronchoscopy: A summary of publications prepared as part of the dissemination of ACCP lung cancer guidelines suggests that for lesions smaller than 2 cm, the sensitivity of bronchoscopy is only 34%.33 Bronchoscopic lung biopsy is unreliable for biopsies of small peripheral lesions, and diagnostic yields as low as 14% have been reported for peripheral lesions smaller than 2 cm.34 This has led to recommendations for CT-guided approaches and suggestions that bronchoscopy should be performed only if an air bronchogram is present (not seen in our case) or in centers with expertise in using newer techniques.35
3. Ultrathin bronchoscopy: Bronchoscopes with working channels of 1.2 to 1.7 mm allow insertion of small biopsy forceps. One study targeted peripheral lesions with a mean diameter of 21.7 mm (range, 10 to 40 mm).36 The overall diagnostic yield was 60%, which was incrementally only 8.6% greater than that attained after the use of standard bronchoscopy. In a second phase of this study, 40.6% of patients with lesions measuring 12 to 55 mm (mean, 24.4 mm) and with negative on-site rapid cytology after standard bronchoscopy had a diagnosis confirmed by ultrathin bronchoscopy. In the largest case series published to date, 102 patients with peripheral lung lesions underwent bronchoscopy with a 3.5 mm thin bronchoscope with a 1.7 mm working channel.37 Transbronchial biopsies (1.5 mm forceps) and bronchial washings with 10 to 20 mL of saline were performed under fluoroscopic guidance. An overall diagnostic yield of 69% was attained in lesions measuring between 1.1 and 7.6 cm (mean, 3.4 cm).
4. Electromagnetic navigational bronchoscopy (ENB): This technique uses an electromagnetic field to track a locatable guide in real time, correlating its position in the airways with a patient’s CT scan. A path to a peripheral lung lesion can be planned and the locatable guide advanced toward it with the use of a steerable probe through the working channel of a standard bronchoscope. Once the guide has reached the lesion, it is removed, leaving a guide sheath (GS) in place through which forceps, brushes, or needles can be advanced. Data from a total of 285 patients showed diagnostic yields between 59% and 77% overall, and between 54% and 75% in nodules measuring 3 cm or less.30 Actual yields may be lower given concerns with study design; inclusion of nonspecific benign features is confirmed only by clinical follow-up, but they are included in the definition of positive results. Another concern pertains to the high cost of disposables. At the time of this writing, the list price of an ENB system is $150,000 or more with various other charges.38 The ENB system has been found to be safe, however, with an average pneumothorax rate of less than 3%. It appears particularly effective in patients whose lesion size and location are beyond those ensuring effectiveness of conventional white light bronchoscopy, who have a history of nondiagnostic procedures, and who are not surgical candidates or are not medically suitable for transthoracic needle aspiration or surgery.
5. High-frequency endobronchial ultrasonography: Radial-type 20 MHz ultrasound probes with outer diameters of 1.4 mm and 1.8 mm coupled with corresponding guiding sheaths, which can fit into 2.0 mm and 2.8 mm working channels, respectively, can be used to visualize pulmonary nodules (current cost in the United States ranges from $3000 to $6000, but probes can potentially last for 50 to 75 examinations).39 These guide a needle, forceps, or brush placed through the sheath to perform the biopsy. EBUS-guided biopsies of peripheral pulmonary lesions improve accuracy and sensitivity compared with conventional transbronchial biopsies; improved sensitivity is most apparent in smaller peripheral lesions, and when the EBUS probe is seen within rather than adjacent to the lesion.30 Investigators have compared 140 prospective EBUS-GS bronchoscopies versus a retrospective analysis of 121 CT-TTNA procedures performed in the same institution during the same time period. Although lesion size was slightly smaller in the EBUS group (2.9 cm vs. 3.7 cm), the overall diagnostic sensitivity was similar (EBUS 66% and CT-TTNA 64%).40 EBUS-GS had higher sensitivity for lesions not touching the visceral pleura compared with lesions touching the visceral pleura (74% vs. 35%). Rates of pneumothorax and tube thoracostomy were significantly greater in the CT-TTNA group compared with the EBUS-GS group (28% vs. 1% for pneumothorax; 6% vs. 0% for tube thoracostomy; P < .001), and fewer pneumothoraces were observed in the CT-TTNA group when lesions were pleural based (2.6% vs. 31.7%). These results suggest that pleural-based lesions are preferably accessed using CT-TTNA, given the low risk of pneumothorax and the poor yield of EBUS in this setting.
6. Multimodal bronchoscopic approach: Some systems provide bronchoscopists with information on the best path to take, offer the ability to take that path, and confirm that the destination has been reached.30 The combination of ENB, which offers maneuverability and the path to the nodule, and EBUS, which confirms that the destination has been reached, has been the subject of a randomized trial. Once the GS position is confirmed via EBUS to be in the lesion of interest, the ultrasound probe is removed and a biopsy forceps advanced to the correct location. In a three-way study design, 118 patients with peripheral lung lesions (mean size, 2.6 cm) underwent ENB, EBUS, or a combination of techniques using diagnostic yield as the primary outcome measure.41 Diagnostic yields for ENB (59%), EBUS (69%), and the combination (88%) were statistically significant. The NPV for combined ENB and EBUS was 75%, which is similar to that for CT-TTNA.33
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


