EBSTEIN’S ANOMALY OF THE TRICUSPID VALVE
Introduction
Ebstein’s anomaly accounts for 0.3% to 0.6% of all congenital heart defects. Ebstein’s anomaly of the tricuspid valve (TV) is characterized by downward (apical) displacement of insertion of posterior and septal leaflets of the TV. As a result, there is tricuspid regurgitation and right atrial enlargement of varying degrees.1 No single gene defect has been identified as a cause. The role of maternal lithium therapy during pregnancy was considered as a cause of Ebstein’s anomaly, but is being disputed recently.2,3 Most cases are sporadic. There is a higher incidence for recurrence in the offspring of women (6%) than that seen in the offspring of men (0.6%) affected by Ebstein’s anomaly.4
Pathology
Central pathology is downward (or apical) displacement of insertion of septal and posterior leaflets of TV from the annulus level. This displacement makes a portion of the right ventricle (RV) to become part of the right atrium (RA; “atrialized” portion of RV [aRV]). As a result, RV distal to displaced insertion of the TV is smaller and lacks some of the inlet portion. The third (anterior) leaflet of the TV in this lesion usually is large, sail-like, and redundant. However, still the coaption of these leaflets is inadequate, leading to varying degrees of tricuspid regurgitation. Persistent tricuspid regurgitation, starting in fetal life in some cases, leads to right atrial enlargement. In some patients, RV outflow tract (RVOT) may be obstructed by the large, redundant anterior leaflet of TV or its chordal attachments,5,6 or there may be true pulmonary stenosis (PS) or atresia.
In severe cases of Ebstein’s anomaly, functional portion of RV may be too small to generate enough systolic pressure that can open the pulmonary valve (PV). Therefore, there may be associated, functional PV atresia, especially in immediate neonatal period when there is transient pulmonary hypertension. If such RV dysfunction occurs in early fetal life, the PV leaflets may fuse before birth, resulting in anatomic atresia rather than functional.7,8
Presence of accessory conduction pathway between atrium and ventricle is common in Ebstein’s anomaly (30%), manifesting either as Wolf–Parkinson–White (WPW) syndrome or with SVT from a concealed pathway. There is also an increased tendency to develop complete atrioventricular (AV) block in this condition.9–11
Other associated lesions include patent foramen ovale (PFO), atrial septal defect (ASD), ventricular septal defect (VSD), patent ductus arteriosus (PDA), tetralogy of Fallot (TOF), double-outlet right ventricle (DORV), mitral valve prolapse or stenosis, transposition of the great arteries (TGA), noncompaction of myocardium, and absent pulmonary valve (APV) syndrome.12
Clinical Features
Variable severity of anatomic and physiologic abnormalities in Ebstein’s anomaly leads to different clinical presentations.
Symptoms
Severe cases of Ebstein’s anomaly may cause fetal hydrops, and such cases carry a high chance of fetal demise.13 After birth, neonatal presentation will depend upon severity of the anomaly. Mild forms of Ebstein’s anomaly are asymptomatic. Severe cases will be associated with significant cardiomegaly and lung hypoplasia. These babies present with cyanosis.14,15 Cyanosis results from right-to-left shunt across PFO/ASD secondary to high pulmonary vascular resistance (PVR) at birth. When the functional portion of the RV is diminished, along with significant tricuspid regurgitation, RV is unable to overcome PVR at birth. This leads to higher right-to-left shunt via PFO and diminished pulmonary blood flow (PBF) resulting cyanosis. Cyanosis may be temporarily improved by keeping the PDA open using prostaglandin (PG) infusion. As the PVR decreases over several days, cyanosis will improve in cases of moderate severity with improved forward flow from RV and decreasing right-to-left shunt across PFO. Thus, transient cyanosis in neonatal period is a typical presentation in Ebstein’s anomaly of moderate severity. Very severe cases of Ebstein’s anomaly will not show such spontaneous improvement with time; but will need neonatal surgical intervention. Fortunately, this will be a small proportion of the babies that need neonatal intervention. Cyanosis is the presenting symptom in 74% of babies. Other presentations include heart failure, incidental murmur, and arrhythmias.15
Physical Examination
Physical examination findings also vary with severity of Ebstein’s anomaly. In mild cases, there may be only multiple heart sounds, presumed to be secondary to the large, anterior TV leaflet. In moderate cases, there may be a murmur of tricuspid insufficiency and mild cyanosis without respiratory distress. In severe cases, features of heart failure, hyperdynamic precordium and holosystolic murmur of tricuspid regurgitation, heard best at the left lower sternal border, are found.
Noninvasive Evaluation
Chest X-Ray
In moderate and severe cases, severe cardiomegaly is the striking feature, secondary to right atrial enlargement (Figure 35.1). In milder cases, cardiac silhouette may be closer to normal. Lung fields are either normal or oligemic.
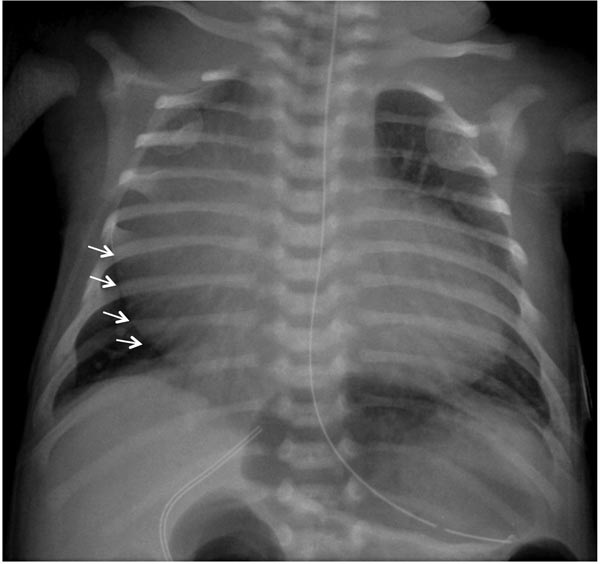
Figure 35.1. Chest x-ray of a neonate with Ebstein’s anomaly. X-ray shows severe cardiomegaly secondary to right atrial enlargement (arrows). Pulmonary vascular markings appear normal in this example although pulmonary oligemia is more typical in severe Ebstein’s anomaly.
Severe cardiomegaly due to right atrial enlargement along with pulmonary oligemia in a cyanotic newborn is unique to Ebstein’s anomaly. But, similar clinical picture may occur with critical PS or pulmonary atresia with intact ventricular septum (PA-IVS) and rarely tricuspid atresia when there is associated obstruction at PFO level causing severe right atrial enlargement. Echocardiography will differentiate these conditions from Ebstein’s anomaly.
ECG
Right atrial enlargement is typically seen in most babies with Ebstein’s. Prolongation of PR interval is noted in two-third of the neonates with Ebstein’s anomaly.16,17 Features of WPW syndrome with short PR interval are reported with a frequency of 30% in Ebstein’s anomaly while a few (12%) have evidence of preexcitation with normal PR interval11 (Figures 35.2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


