Earlobe crease (ELC) has been linked to coronary artery disease; however, systematic evaluations of the earlobe and its relation to ischemic stroke are lacking. The objectives were to define the ELC using a single-blind approach and to determine through multivariate analysis its association with cardiovascular events (CVEs) comprising coronary, ischemic cerebrovascular, and peripheral vascular diseases. A single-blind cross-sectional study was performed in 2 phases: (1) an initial study (n = 300) to define ELC classification criteria and (2) a confirmation stage (n = 1,000) to analyze ELC association with CVEs. Each of the participants’ pinnae were photographed and classified blindly by joint decision according to ELC’s inclination, length, depth, and bilateralism. Patients’ medical histories were reviewed for age, cardiovascular risk factors, and CVEs. The concordance rate after the classification of all photographs was 89.6%. The first phase did not find any correlation between the different depth degrees or vertical creases and CVEs. The second stage concluded that diagonal bilateral ELC prevalence in patients with CVEs was 43% compared with 29% in the control patients (p <0.001). The multivariate analysis showed an association between ELC and CVEs (odds ratio 1.45, 95% confidence interval [CI] 1.08 to 1.93, p = 0.012), with a sensitivity and specificity of 43% and 70%, respectively. Ischemic stroke alone was also associated with diagonal bilateral ELC (odds ratio 1.67, 95% confidence interval 1.1 to 2.51, p = 0.015). In conclusion, diagonal bilateral ELC is independently associated with CVEs in the hospitalized population. An independent association with ischemic stroke has also been demonstrated for the first time.
Prevention of cardiovascular disease is based on the identification of high-risk subjects, so easily detectable physical signs, such as waist circumference (WC) or ankle-brachial index (ABI), are useful to recognize occult atherosclerosis. However, the earlobe crease (ELC), a simple sign assessable with nothing more than a quick glance, that was linked to coronary artery disease (CAD) decades ago, has largely been ignored. It is a line covering at least 1/3 of the length between the tragus and the posteroinferior lobe edge. A number of studies have confirmed its association with CAD or peripheral vascular disease, but its relation with ischemic stroke has not yet been explored. As far as a nonbiased analysis of ELC and its variability is lacking, and a minority of reports have controlled confounders like age, the aims of this study were to (1) define the ELC through a single-blind approach, hiding the patient’s case-control status when evaluating the ELC and exploring each ELC characteristic separately to analyze which one was the most determinant in the association with cardiovascular events (CVEs); and (2) use multivariate analysis controlling for factors such as age to determine ELC’s effect on CVEs, comprising not only CAD but also peripheral vascular and ischemic cerebrovascular diseases and its ability to predict CVEs.
Methods
Patients >18 years admitted to the medical wards of the Hospital Universitario La Paz, Madrid, Spain, from March 15, 2014, to June 15, 2014, were eligible to participate in this cross-sectional study. The protocol and consent procedure were approved by the institutional ethics committee in accordance with the European guidelines for good clinical practice and with the ethical guidelines of the 1975 Declaration of Helsinki. The patients were informed about the study, and written consent was obtained before inclusion.
The study was divided into 2 phases: (1) the first phase enrolled 300 patients to typify the various ELC features, determining the sensitivity, specificity, and predictive values of each characteristic in detecting atherosclerosis; (2) the second phase enrolled 700 additional patients, bringing the total sample to 1,000 patients, using the classification criteria previously determined for the first phase.
After signing the informed consent, the patients had both pinnae photographed by a researcher who assigned to each participant an identification number attached to their photographs, which remained linked to their medical record number in a protected database to ensure data confidentiality. To preserve the blinding, a different researcher reviewed the medical record of each patient for their birth date, gender, coronary risk factors, history of myocardial infarction, coronary revascularization, stroke, transient ischemic attack (TIA), atrial fibrillation, carotid stenosis, aortic aneurysm, aortic dissection, lower limb vascular disease, cancer, and laboratory data.
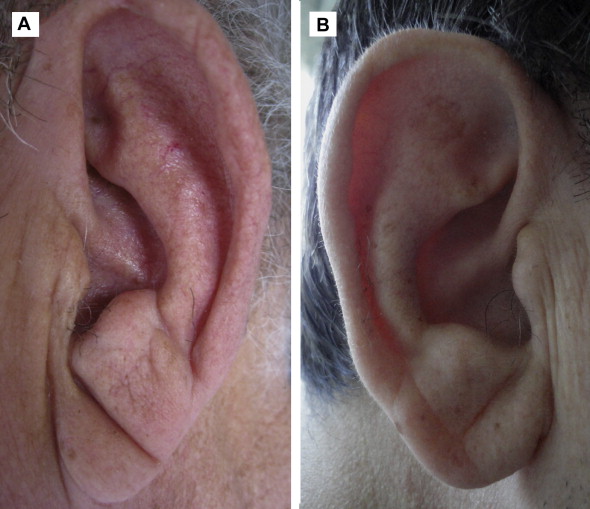
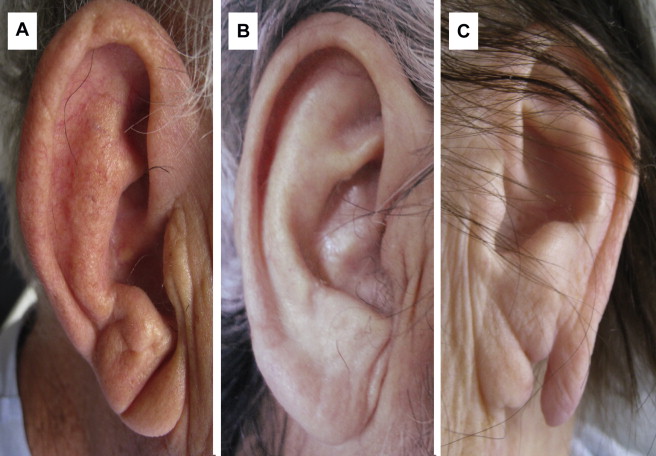
Finally, all pinnae were classified by consensus among 3 researchers. Discrepancies were solved by consensus with the participation of a fourth researcher. Each photograph was classified according to the following characteristics: length, depth, bilateralism, and inclination. Length ( Figure 1 ) was qualified as complete when the line crossed the entire distance from the tragus to the earlobe’s edge ( Figure 1 ) and incomplete when it crossed >1/3 of the earlobe without reaching the border ( Figure 1 ). Depth ( Figure 2 ) was qualified as mild when it faintly insinuated ( Figure 2 ), moderate when it marked a fold where the end could be appreciated ( Figure 2 ), and severe when the end of the fold could not be seen ( Figure 2 ). The ELC was considered bilateral when any line appeared in both ears and unilateral if it only appeared in 1. Finally, 2 creases referring to the inclination were defined ( Figure 3 ): a diagonal crease that extended from the tragus posterolaterally or inferiorly to the lobe ( Figure 3 ) and a vertical crease that ended anteromedially to this site after running close and parallel to the lobe medial edge ( Figure 3 ). Earlobes where the presence of the crease could not be determined were considered as ELC negative ( Figure 3 ).

The continuous variables are presented as mean ± SD and were compared using Student’s t test; the categorical variables were compared using the chi-square test or Fisher’s exact test. The concordance rate after the photograph classification was estimated from the number of photographs about which any of the 3 investigators disagreed. The Cochrane-Armitage trend test was applied for analysis between different ELC types and CVEs. Sensitivity, specificity, and predictive values were calculated from the contingency tables of ELC-CVEs. The effect was quantified by univariate and multivariate logistic regression models. All the variables were modeled categorically using dummy variables. Statistical significance was set at p <0.05. The data were analyzed at the Hospital Universitario La Paz with SPSS 18.0 (Chicago, Illinois) for Windows.
Results
Patients of both stages were comparable at sociodemographic, lifestyle, and clinical characteristics. Baseline characteristics of the total sample are listed in Table 1 .
| Variable | All (n=1000) | Bilateral ELC | p | |
|---|---|---|---|---|
| Yes (n = 349) | No (n = 651) | |||
| Male | 573 (57%) | 196 (56%) | 377 (58%) | 0.59 |
| Age, years ± SD | 67.5 ± 16.5 | 74.4 ± 11.3 | 63.7 ± 17.6 | < 0.001 ∗ |
| Familiar history of early AMI | 109 (11%) | 40 (11%) | 69 (11%) | 0.68 |
| Hypertension | 636 (64%) | 253 (72%) | 383 (59%) | <0.001 ∗ |
| Diabetes mellitus | 286 (29%) | 129 (37%) | 157 (24%) | <0.001 ∗ |
| Hypercholesterolaemia | 451 (45%) | 179 (51%) | 272 (42%) | 0.004 ∗ |
| Hypertriglyceridemia | 55 (5%) | 15 (4%) | 40 (6%) | 0.22 |
| Smoker | 483 (48%) | 159 (45%) | 324 (50%) | 0.2 |
| Coronary heart disease | 263 (26%) | 114 (33%) | 149 (23%) | 0.001 ∗ |
| Ischaemic stroke | 130 (13%) | 67 (19%) | 63 (10%) | <0.001 ∗ |
| Hemorrhagic stroke | 26 (3%) | 10 (3%) | 16 (2%) | 0.7 |
| Transient ischaemic attack | 61 (6%) | 26 (7%) | 35 (5%) | 0.19 |
| Atrial fibrillation | 222 (22%) | 86 (25%) | 136 (21%) | 0.17 |
| Carotid artery stenosis | 44 (4%) | 23 (7%) | 21 (3%) | 0.013 ∗ |
| Lower limb vascular disease | 52 (5%) | 23 (7%) | 29 (4%) | 0.15 |
| Aortic aneurism | 26 (3%) | 7 (2%) | 19 (3%) | 0.39 |
| Aortic dissection | 3 (0.3%) | 0 | 3 (0.5%) | 0.2 |
| Cancer | 174 (17%) | 64 (18%) | 110 (17%) | 0.57 |
| ACE inhibitors | 352 (35%) | 134 (38%) | 218 (33%) | 0.12 |
| ARBs | 175 (17%) | 68 (19%) | 107 (16%) | 0.23 |
| Diuretics | 455 (45%) | 168 (48%) | 287 (44%) | 0.22 |
| Vasodilators | 184 (18%) | 79 (23%) | 105 (16%) | 0.011 ∗ |
| β-blockers | 427 (43%) | 168 (48%) | 259 (40%) | 0.011 ∗ |
| Insulin | 121 (12%) | 62 (18%) | 59 (9%) | <0.001 ∗ |
| Oral hypoglycemic agents | 187 (19%) | 80 (23%) | 107 (16%) | 0.012 ∗ |
| Statins | 510 (51%) | 208 (60%) | 302 (46%) | <0.001 ∗ |
| Fibrates | 22 (2%) | 8 (2%) | 14 (2%) | 0.88 |
| Haemoglobin (g/dL) | 13.1 ± 3.57 | 13 ± 5.28 | 13.1 ± 2.17 | 0.12 |
| Haematocrit (%) | 40 ± 6.1 | 39.5 ± 6.05 | 40.3 ± 6.06 | 0.45 |
The frequency of each pinna characteristic found during the first phase is listed in Table 2 . The first Cochran-Armitage trend analysis ( Figure 4 ) revealed a lack of association between vertical creases and CVEs; thus, the other features were detailed only for diagonal creases. ELC will hereafter refer exclusively to diagonal creases. No association was found between the depth degrees and CVEs; this category was, therefore, discounted. The characteristics of bilateralism and length, always referring to diagonal ELC, were selected for the second phase to analyze the total sample.
| Inclination (n=600) | No crease | 45 % |
| Diagonal | 41 % | |
| Vertical | 14 % | |
| Bilateralism (n=300) | No diagonal crease | 50 % |
| Unilateral | 18 % | |
| Bilateral | 32 % | |
| Length (n=600) | No diagonal crease | 59 % |
| Incomplete | 6 % | |
| Complete | 34 % | |
| Depth (n=600) | No diagonal crease | 59 % |
| Mild | 14 % | |
| Moderate | 17 % | |
| Severe | 9 % |
Diagonal bilateral ELC was associated with CVEs, which comprised coronary heart disease (acute myocardial infarction or coronary revascularization), ischemic cerebrovascular disease (ischemic stroke or TIA), and peripheral vascular disease (intermittent claudicating, lower limb revascularization surgery, carotid artery stenosis, or carotid endarterectomy). However, none of these 3 cardiovascular conditions achieved statistical significance when analyzed separately. The sensitivity and specificity of bilateral ELC in detecting CVE were 42% and 73%, respectively, with a positive predictive value of 43% and a negative predictive value of 73%.
The concordance rate in the total sample after the classification of all photographs was 89.6%. The selected characteristics of length and bilateralism were analyzed using a Cochran-Armitage trend, which showed that bilateralism, regardless of length, was associated with a higher frequency of CVEs (p <0.001; Figure 5 ). Thus, all subsequent analyses will refer only to bilateral diagonal ELC. The baseline characteristics of the sample and their association with bilateral ELC determined by the chi-square test are listed in Table 1 . Some 53% of the patients had an ELC on least 1 ear, whereas the prevalence of bilateral ELC was 35%, which is more common in elder, hypertensive, diabetic, or hypercholesterolemic patients.
The prevalence of CVEs was 41% (26% coronary heart disease, 17% ischemic cerebrovascular disease, and 9% peripheral vascular disease). The frequency of bilateral ELC in patients with CVEs was 43%, whereas 29% of the healthy subjects had bilateral ELC (p <0.001). Associations between these conditions and known risk factors after the chi-square test and univariate regression are listed in Table 3 : bilateral ELC was significantly associated with all 3 vascular diseases and with hypertension, diabetes, and hypercholesterolemia.
| Coronary heart disease | Ischaemic cerebrovascular disease | Peripheral vascular disease | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Male | 2.59 (1.9-3.53) | <0.001 | 0.94 (0.73-1.41) | 0.9 | 1.92 (1.18-3.11) | 0.008 |
| Age (</> 70 years) | 1.2 (0.91-1.59) | 0.2 | 3.46 (2.39-5) | <0.001 | 1.55 (0.99-2.43) | 0.057 |
| Familiar history of early AMI | 1.9 (1.25-2.88) | 0.002 | 0.75 (0.42-1.32) | 0.31 | 0.95 (0.46-1.96) | 0.89 |
| Hypertension | 2.31 (1.68-3.19) | <0.001 | 2.93 (1.95-4.41) | <0.001 | 3.19 (1.77-5.74) | <0.001 |
| Diabetes mellitus | 2.04 (1.51-2.75) | <0.001 | 1.89 (1.34-2.65) | <0.001 | 2.62 (1.67-4.1) | <0.001 |
| Hypercholesterolaemia | 2.32 (1.67-2.97) | <0.001 | 1.94 (1.39-2.71) | <0.001 | 3.49 (2.14-5.69) | <0.001 |
| Smoker | 1.61 (1.21-2.14) | 0.001 | 0.8 (0.57-1.11) | 0.18 | 1.46 (0.94-2.29) | 0.09 |
| Atrial fibrillation | 0.93 (0.66-1.31) | 0.68 | 2.28 (1.59-3.25) | <0.001 | 1.07 (0.63-1.8) | 0.8 |
| Carotid artery stenosis | 1.32 (0.69-2.54) | 0.4 | 38.85 (16.11-93.68) | <0.001 | – | – |
| Bilateral ELC | 1.63 (1.22-2.18) | 0.001 | 1.97 (1.41-2.75) | <0.001 | 1.7 (1.09-2.66) | 0.019 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


