Dyspnea has been variously described as the sensation of breathlessness or of difficult or uncomfortable breathing. One consensus statement defined dyspnea as
… a term used to characterize a subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity. The experience arises from interactions among multiple physiological, psychological, social, and environmental factors and may induce secondary physiological and behavioral responses (1).
Some degree of dyspnea is normal at high altitude or in the context of vigorous exercise; dyspnea is abnormal when it occurs at levels of activity and in environmental circumstances for which normal individuals would not be breathless. The severity of dyspnea that an individual experiences for a given activity appears to be related to the level of ventilation required for that activity in relation to the ventilatory capacity of the individual.
Breathlessness is an extremely common complaint. In one large study of medical outpatients, it was the third most frequent complaint, following only fatigue and back pain (2). Dyspnea is the usual presenting symptom for some of the most common chronic conditions afflicting Americans, including chronic obstructive lung disease (14 million people), asthma (10 million individuals), and heart failure (5 million Americans). It is a prominent symptom in nearly all other pulmonary disorders and may be the presenting symptom in patients with coronary artery disease.
USUAL CAUSES
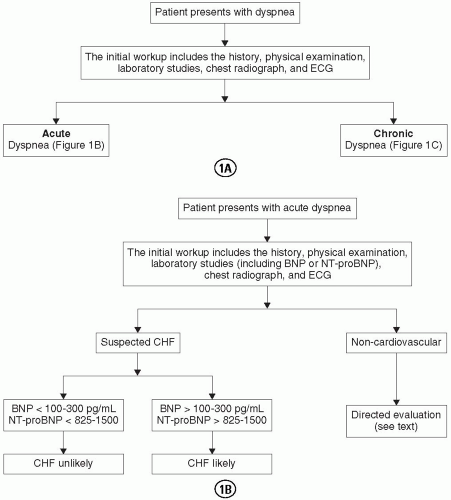
Dyspnea can be divided into acute and chronic dyspnea. Acute dyspnea develops over minutes to days. It usually results from an acute cardiovascular or pulmonary process and, as such, mandates urgent diagnostic evaluation and treatment. Cardiovascular conditions precipitating acute dyspnea include myocardial or valvular abnormalities that cause pulmonary edema (e.g., myocardial ischemia or infarction, acute mitral or aortic regurgitation), hypertensive urgency or emergency, pericardial tamponade, and pulmonary artery thromboembolism. Pulmonary abnormalities include pneumonia, asthma or other reactive airway disease, pneumothorax, upper airway obstruction, or diffuse lung injury as a manifestation of the systemic inflammatory response syndrome. Overdoses of aspirin or ethylene glycol may cause dyspnea by direct stimulation of the respiratory center. Fortunately, the cause of acute dyspnea can usually be determined from a history, a physical examination, basic laboratory studies, a chest radiograph, and an electrocardiogram, with other testing as indicated [e.g., cardiac enzyme levels for myocardial infarction, ventilation/perfusion lung scanning for pulmonary embolism, transesophageal echocardiography for proximal aortic dissection with aortic insufficiency, and peak flow for acute airway disease (3,4)] (Fig. 2.1A and B).
Increasingly, natriuretic peptides have assumed a central role in the evaluation of acute dyspnea. These peptides are produced and released by cardiac myocytes (5). B-type natriuretic peptide (BNP) is produced and released almost exclusively by the ventricular myocardium in response to an elevation in end-diastolic pressure and volume (6). The pro-peptide circulates and is cleaved into a biologically active fragment and the N-terminal pro-B-type natriuretic peptide (NT-proBNP) (7). Assays for BNP and NT-proBNP are available and exhibit different operating characteristics (7,8), although they correlate closely in dyspneic patients (9). The NT-proBNP has a longer plasma half-life and considerably higher concentrations (7). Importantly, in normal subjects and heart failure patients, intraindividual coefficients of variation may vary between 24% and 77%, albeit with generally lower levels in stable patients. In addition, plasma BNP and NT-proBNP increase with advancing age and female gender (10,11), as well as with renal insufficiency and hypertension (12,13). Numerous investigators have examined the role of natriuretic peptide concentration in identifying heart failure as the cause of acute dyspnea. A large, multicenter, emergency department-based study confirmed the benefit in 1,586 patients evaluated for acute dyspnea (4). Additional studies have confirmed the value of BNP or NT-proBNP level measurement in acutely dyspneic patients of varying age and gender (14,15,16,17). The threshold value for defining normality in these studies has varied with the assay and study population; generally, BNP values of 100 to 300 and NT-proBNP values of 825 to 1,500 have been used. In general, peptide levels provide the greatest diagnostic accuracy in identifying heart failure in acutely dyspneic patients (18). The most compelling data come from a recent, randomized study of patients evaluated in the emergency department for acute dyspnea; the use of BNP in clinical decision making reduced the need for hospital admission (85% to 75%), the need for intensive care (24% to 15%), and reduced the length of hospitalization (11 days to 8 days) (19). The mean total cost of treatment was lower in the BNP-managed group.
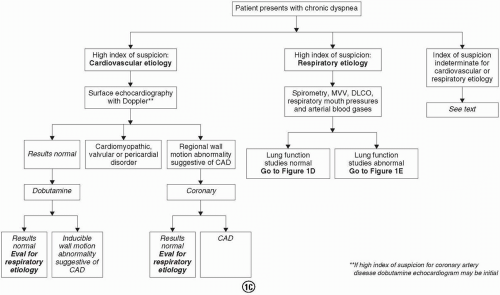
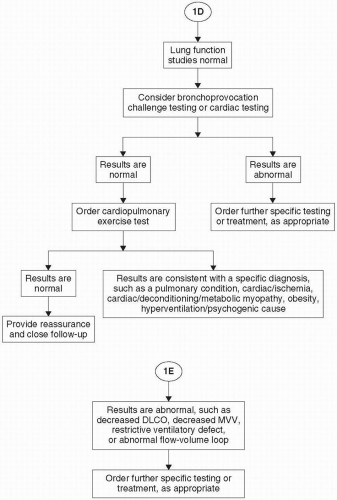
FIGURE 2.1. Evaluation for patients first seen with dyspnea. (From: Martinez F. Evaluation of Dyspnea: Educational Review Manual in Pulmonary Disease. New York: Castle Connolly Graduate Medical Publishing, 2003.) (continued)
FIGURE 2.1.(Continued)
FIGURE 2.1.(Continued)
Chronic dyspnea (symptoms present for at least a month) often represents a greater diagnostic challenge and is the focus of the remainder of this chapter. Table 2.1 provides a pathophysiologic framework for the causes of chronic dyspnea, along with specific examples. The causes can be conveniently divided into those characterized by impaired cardiovascular function, by impaired pulmonary function, or by abnormally altered central ventilatory drive or perception. An evaluation is illustrated in Figs. 1C through E.
Impaired Cardiovascular Function
Any condition that increases left atrial pressure results in a concomitant increase in pulmonary venous pressure, with vascular congestion and decreased pulmonary compliance. Left atrial pressure increases in patients with elevated left ventricular end-diastolic pressure, whether the latter results from systolic dysfunction (e.g., ischemic or nonischemic cardiomyopathies), diastolic dysfunction (e.g., hypertensive heart disease with left ventricular hypertrophy, hypertrophic cardiomyopathy, or restrictive cardiomyopathy), or an obstruction to left atrial emptying (e.g., mitral stenosis). More profound or acute elevations in pulmonary venous pressure lead to alveolar filling with impaired gas exchange and arterial hypoxemia. Bronchial hyperresponsiveness (i.e., “cardiac asthma”) occurs in some individuals in this setting. If the ability to increase cardiac output with exercise is reduced (e.g., left ventricular systolic dysfunction, aortic stenosis), oxygen delivery is compromised, and lactic acidosis occurs prematurely. Ventilation must increase to eliminate the excess acid, and this may result in dyspnea, even in the absence of pulmonary congestion.
Coronary artery disease (CAD) is an important and often unrecognized cause of dyspnea in patients with normal left ventricular systolic function at rest. Chest pain may be absent in such patients (e.g., many diabetics), for whom dyspnea is the “anginal equivalent.” Transient ischemia resulting from increased metabolic demand, heightened coronary vascular tone, or coronary microthrombi may cause papillary muscle dysfunction with acute mitral regurgitation, systolic dysfunction, or diastolic dysfunction.
Dyspnea is a prominent symptom in patients with pericardial and pulmonary vascular disease, even when oxygenation and lung mechanics are normal. The mechanism underlying dyspnea in these settings probably is related to activation of stretch receptors or baroreceptors in the central circulation.
Congenital cardiac anomalies also may manifest with dyspnea. Anatomic abnormalities resulting in right-to-left shunts cause hypoxemia. This stimulates arterial chemoreceptors, which in turn activate respiratory control centers to increase ventilation. Leftto-right shunts, if sufficiently large, will over time result in left ventricular volume overload and progressive systolic dysfunction. In some patients, increased flow though the pulmonary vasculature results in adverse pulmonary vascular remodeling and consequent pulmonary hypertension.
Impaired Pulmonary Function
Conditions that obstruct airflow, whether diffuse [e.g., asthma, chronic obstructive pulmonary disease (COPD)] or focal (e.g., vocal cord paralysis, tracheal stenosis, endobronchial tumor), result in dyspnea. Increased work of breathing is typically noted in these conditions. Heterogeneous reduction of airflow, when present, results in regional ventilation/perfusion mismatching, with consequent hypoxemia and increased ventilatory requirements. However, ventilatory muscle fatigue and air trapping reduce ventilatory capacity.
TABLE 2.1.Pathophysiologic framework for chronic dyspnea, with specific examples
CATEGORY
EXAMPLE
Impaired cardiovascular function
Myocardial disease
Systolic dysfunction
Ischemic cardiomyopathy
Nonischemic cardiomyopathies
Diastolic dysfunction
Hypertensive heart disease
Coronary artery disease
Hypertrophic cardiomyopathy
Restrictive cardiomyopathy
Valvular disease
Aortic or mitral regurgitation
Aortic or mitral stenosis
Pericardial disease
Constrictive pericarditis
Pulmonary vascular disease
Pulmonary thromboembolism
Primary pulmonary hypertension
Congenital anomalies
Cyanotic heart diseases (right-to-left shunts)
Impaired pulmonary function
Airflow obstruction
Diffuse
Asthma
COPD
Focal
Vocal cord dysfunction or paralysis
Tracheal stenosis
Endobronchial tumor
Restriction of lung mechanics
Interstitial lung disease
Idiopathic pulmonary fibrosis
Pneumoconioses
Lymphangitic carcinomatosis
Extrapulmonary thoracic restriction
Kyphoscoliosis
Pleural effusion or fibrosis
Neuromuscular weakness
Phrenic nerve paralysis
Spinal cord injury
Amyotrophic lateral sclerosis
Abnormal gas exchange
Abnormal alveoli/capillary interface
Eosinophilic pneumonia
Right to left shunting
Pulmonary arteriovenous malformations
Altered central ventilatory drive or perception
Systemic or metabolic disorders
Increased metabolic requirements
Hyperthyroidism
Obesity
Decreased oxygen-carrying capacity
Anemias
Metabolic acidosis
Renal failure
Mitochondrial myopathies
Direct stimulation of respiratory center
Aspirin or ethylene glycol overdose
Physiologic processes causing dyspnea
Vigorous exercise
Pregnancy
Hypoxic breathing at high altitude
Deconditioning
COPD; chronic obstructive pulmonary disease.
Adapted from Sietsema K. Approach to the patient with dyspnea. In: Humes HD, ed. Kelley’s Textbook of Medicine, 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2000.
Restriction of lung mechanics may result from abnormalities of the lung parenchyma (e.g., idiopathic pulmonary fibrosis), pleural disease, skeletal abnormalities (e.g., kyphoscoliosis), or neuromuscular disorders. The reduction in ventilatory capacity may be exacerbated by an increase in ventilatory requirements that results from ventilation/perfusion mismatching. Abnormal gas exchange may result from abnormalities of the alveolar/capillary interface or from pulmonary right-to-left shunting.
Altered Central Ventilatory Drive or Perception
Hyperthyroidism and obesity increase respiratory drive because of increased metabolic requirements. Anemic patients have reduced oxygen-carrying capacity, which, when severe, increases the respiratory rate. The lactic acidosis accompanying renal failure and mitochondrial myopathies results in compensatory respiratory alkalosis. Respiratory drive is directly stimulated in aspirin toxicity and is a response to the metabolic acidosis that occurs in this setting, as well.
The prevalence of the aforementioned conditions in patients presenting for evaluation of dyspnea probably depends on the patient sample, physician type, and practice setting. Three studies (20,21,22) have catalogued the causes of chronic dyspnea and their frequencies in referral samples (Table 2.2). It is evident that airway diseases, such as asthma or COPD, represented the majority of cases, followed by cardiac disease, interstitial lung disease, deconditioning, psychogenic disorders, gastroesophageal reflux, neuromuscular disease, and pulmonary vascular disease. Referral bias may have influenced these studies, inasmuch as they all originated from pulmonary referral clinics. Cardiologists would probably identify a higher proportion of cardiovascular disease in their practices. A report of patients with a chief complaint of “shortness of breath,” both acute and chronic, seen by general practice physicians in Australia identified the most common diagnoses as asthma, COPD, heart failure, acute bronchitis, hypertension, ischemic heart disease, anxiety, and upper respiratory tract infections (23).
TABLE 2.2.Etiology of chronic dyspnea in three series of patients studied in tertiary pulmonary clinics