The blood supply to the transverse rectus abdominis myocutaneous (TRAM) flap travels down through the rectus muscle from the continuation of the internal mammary vessels in the chest as the superior epigastric artery and vein. Maintaining this blood supply allows the surgeon to elevate and rotate the flap and transfer it to the chest through a tunnel made over the xiphoid. Once on the chest, it is shaped into the breast mound. Using only one rectus abdominis muscle is called a “single-pedicle flap”; using both muscles is the “double-pedicle flap.” Both of the muscles are used in unilateral reconstruction cases when there is a midline scar in the lower abdomen that blocks blood flow across the scar or when the surgeon feels the need to use all of the tissue from the abdomen to make the appropriate breast size. The disadvantage of this approach is the significant sacrifice in abdominal wall integrity and function. In bilateral pedicled TRAM flap cases, both muscles must be used to supply blood to each side independently.
Pedicled TRAM flaps, particularly the single-pedicled variety, have the least robust blood flow because of the long distance from the origin of the blood supply to the flap. As a result, flaps based on the more dominant perfusion from the inferior epigastric artery system have been developed. However, because the origin of this pedicle is in the pelvis, it tethers the flap in that region and requires that it be disconnected and transferred. This is referred to as a “free flap” because it is temporarily separated from the body before being reattached in a new location. This requires the use of microsurgical techniques to reestablish blood flow to the flap in the area of the breast. The two most common recipient vessels for the free flap are the internal mammary artery and vein adjacent to the sternum and the thoracodorsal pedicle in the axilla.
In order to minimize the functional compromise to the abdominal wall, surgeons have continued to devise new methods to provide the flap with blood flow with little or no muscle sacrifice. These are all microsurgical procedures and include “muscle-sparing” free TRAM flaps in which only a small cuff of muscle is taken with the flap. Also, the deep inferior epigastric perforator (DIEP) and superficial inferior epigastric artery (SIEA) flaps take no muscle with them at all. There has been much discussion among surgeons as to which of these microsurgical options is best. Fundamentally, it comes down to a balance between providing sufficient blood flow to the flap for its complete survival and minimizing the functional insult to the abdominal wall. Each of these operations is a one-time-only proposition and cannot be redone if the tissue does not survive. Consequently, all efforts must be made to maximize the blood flow to the flap, and the risk of outright flap loss should be less than 1%. Marginal blood flow leading to fat necrosis also needs to be rare, because fat necrosis creates hard lumps in the flap that may mimic recurrent cancer. To address these issues, we developed the technique of using color-flow duplex imaging to assess the blood supply of potential flaps for breast reconstruction. The ability to preoperatively map (locate and mark) the arterial perforators on the abdominal wall assists the surgeon in planning the procedure to ensure that the dominant vessels are included in the flap. This evaluation is useful for all of the flaps described in this chapter, but it is most important in those flaps that depend on fewer perforators for their perfusion.
THE VASCULAR LABORATORY AND TRAM FLAP SURGERY
In the 1980s, a series of reports described the intraoperative use of a continuous-wave Doppler device to map the perforator arteries for TRAM flap surgery.1–5 These authors were primarily concerned with identifying variations in the anatomy of the blood vessels and selecting the flap segment most likely to have adequate perfusion. Michelow et al5 evaluated 66 patients undergoing breast reconstruction and found that approximately 80% had a single vascular axis coursing through the rectus abdominis muscle, while nearly 20% displayed two axes (Fig. 36.1). In this patient population, the majority of vascularity was found in the middle third of the rectus abdominis muscle; however, in approximately 28% of the patients, the blood supply was located in the medial or lateral third of the muscle. Many surgeons prefer not to use the entire rectus abdominis muscle in an effort to reduce complications such as postoperative hernias. The goal in a muscle-sparing procedure is to harvest a segment of muscle that has adequate perfusion. Rozen et al6 performed computed tomography angiography (CTA) in eight consecutive patients undergoing flap surgery for breast reconstruction. The CTA results revealed three distinct patterns of deep inferior epigastric artery branching (Fig. 36.2). The majority of perforators are in the region of the umbilicus, but the locations are rarely symmetrical from side to side. The anatomy of the rectus abdominis muscle and perforating arteries is shown in Figure 36.3.
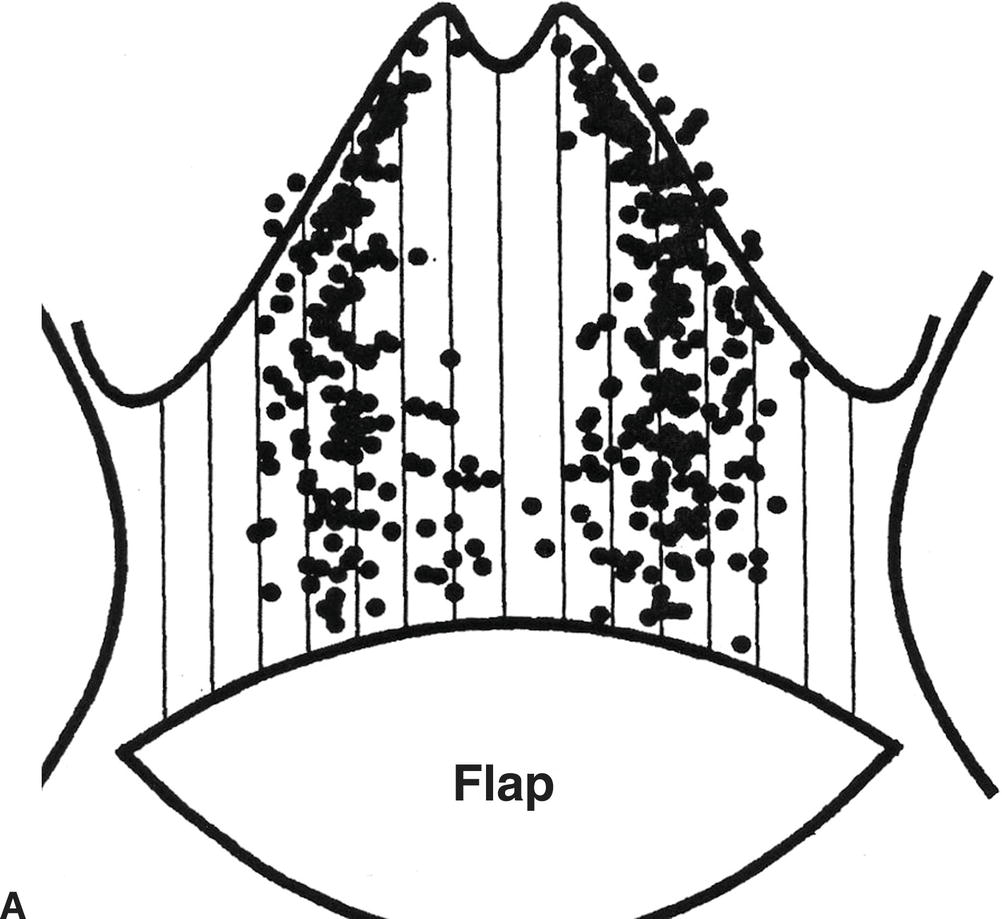
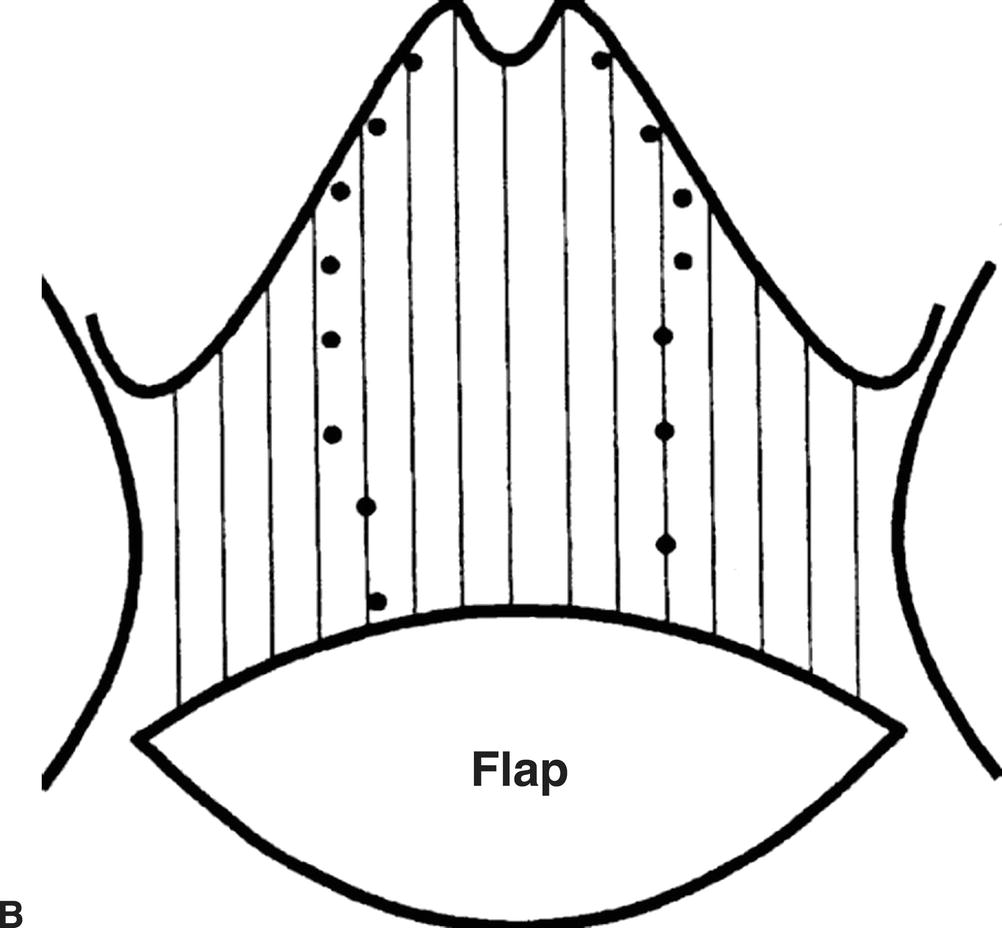
FIGURE 36.1. A,Accumulated scatter diagram of Doppler sound points shows the location of the arterial supply to the rectus abdominis muscles in 66 patients. B,Plotted Doppler sound points indicate the vascular axis of the flap in 129 rectus abdominis muscles.
(From Michelow BJ, Hartrampf CR Jr, Bennett GK. TRAM flap safety optimized with intraoperative Doppler. Plast Reconstr Surg 1990;86:143–146, with permission.)
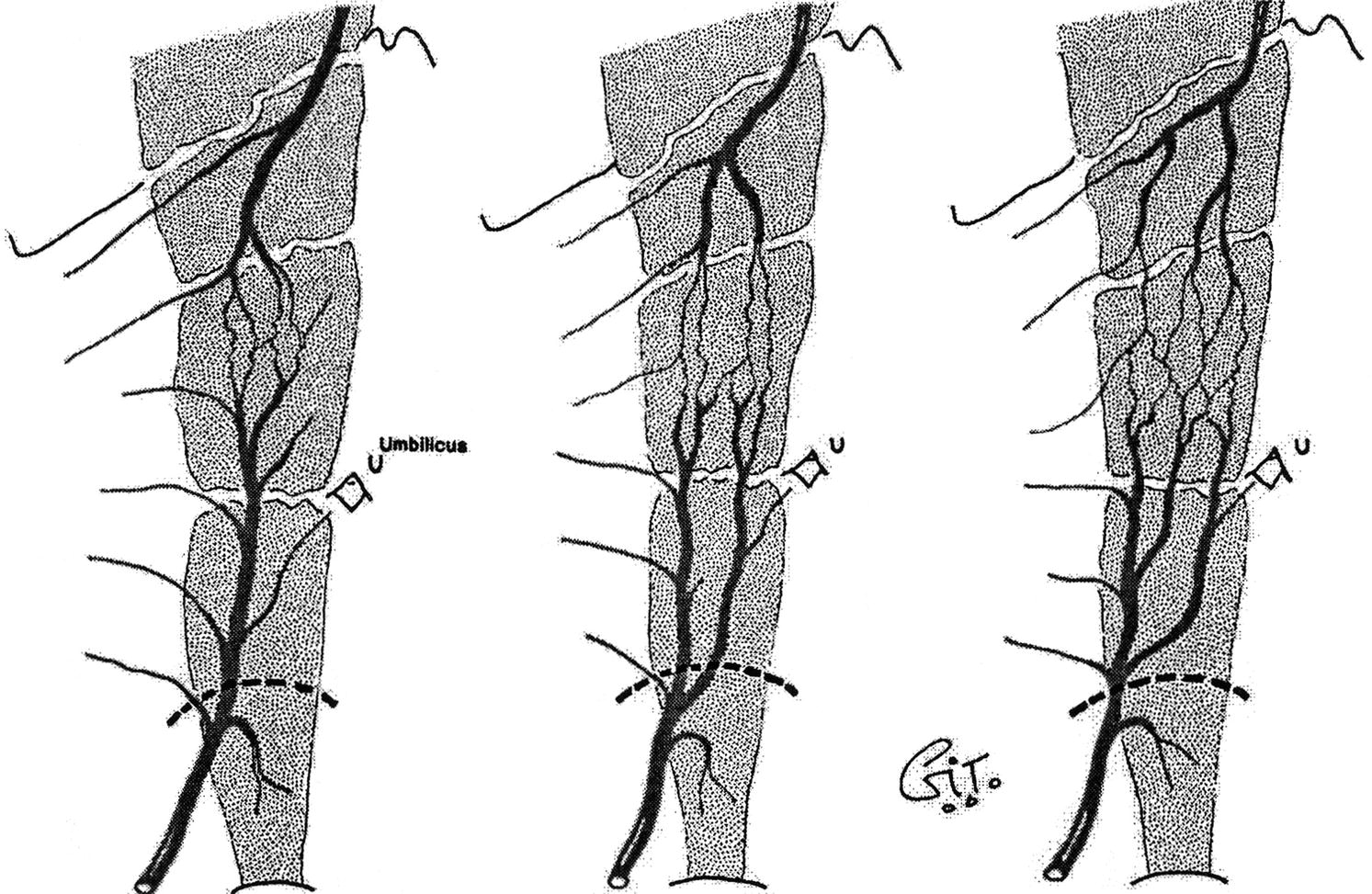
FIGURE 36.2. Three patterns of branching for the deep inferior epigastric artery.
(From Rozen WM, Phillips TJ, Ashton MW, et al. Preoperative imaging for DIEA perforator flaps: A comparative study of computed tomographic angiography and Doppler ultrasound. Plast Reconstr Surg 2008;121:1–8, with permission.)
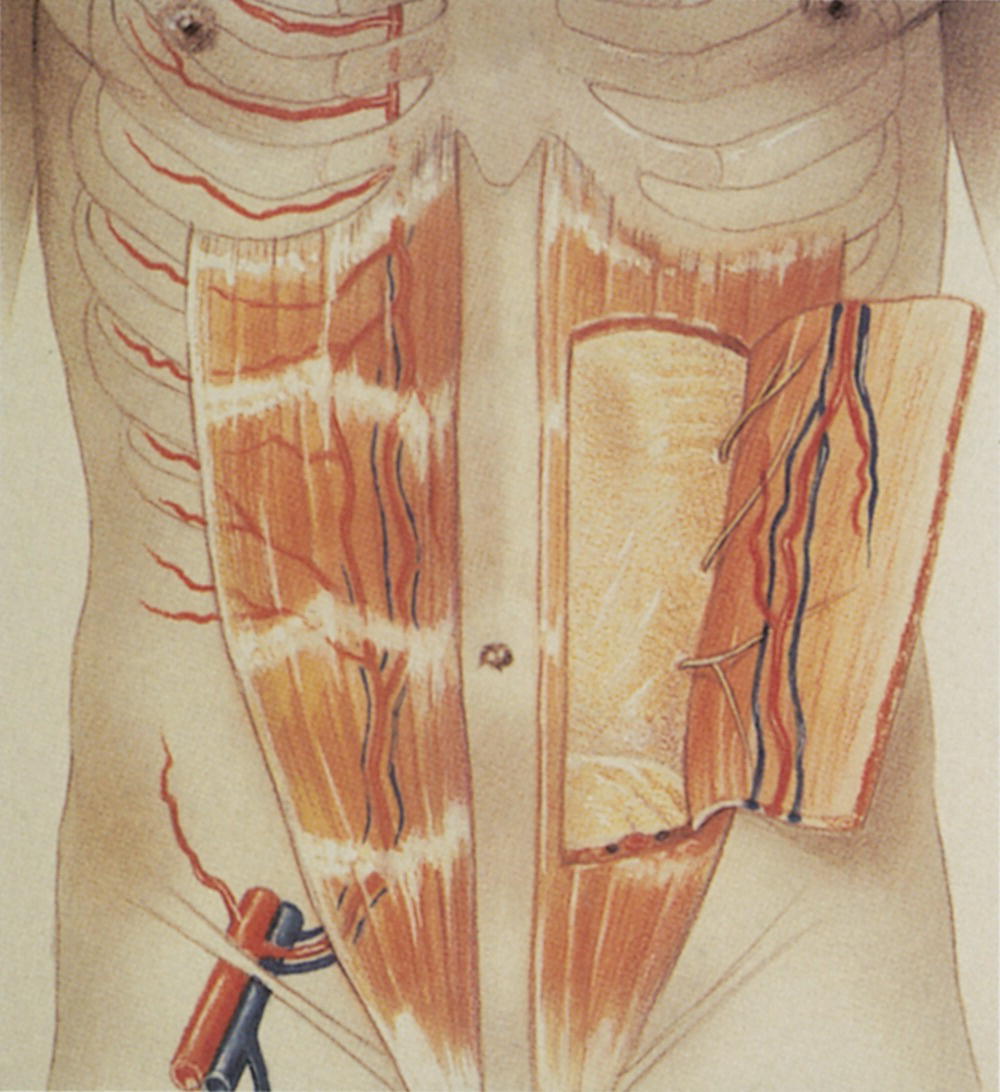
FIGURE 36.3. Origin of the deep inferior epigastric artery from the external iliac artery. It courses up the posterior aspect of the rectus abdominis muscle to anastomose with branches of the superior epigastric artery.
In 1990, Miles Cramer from the vascular laboratory at the University of Washington and Dr. Richard Rand from the University of Washington Division of Plastic Surgery set out to improve on the intraoperative examinations of the early 1980s and introduced preoperative duplex ultrasound imaging to further reduce the risk of tissue loss in breast reconstruction surgery.7 They performed duplex scanning (B-mode imaging, pulsed Doppler spectral analysis, and color-flow Doppler) in 13 patients and 2 normal volunteers (all female) between March and November 1991. Their hypothesis was that duplex scanning would provide more detailed anatomic and physiologic information than the continuous-wave Doppler examinations performed by others. In addition, this critical information could be obtained preoperatively to aid in surgical planning. Cramer et al7 were successful in documenting the following features:
- Patency and continuity of the deep inferior epigastric arteries (Figs. 36.4 and 36.5)
- Patency and continuity of the internal mammary arteries (Fig. 36.6)
- Peak systolic velocities and diameter measurements for the perforator arteries (Fig. 36.7)
- Locations of perforator arteries by zone and side, with reference to the umbilicus
- Ability to mark each perforator artery on the skin with a high level of accuracy (Fig. 36.8)
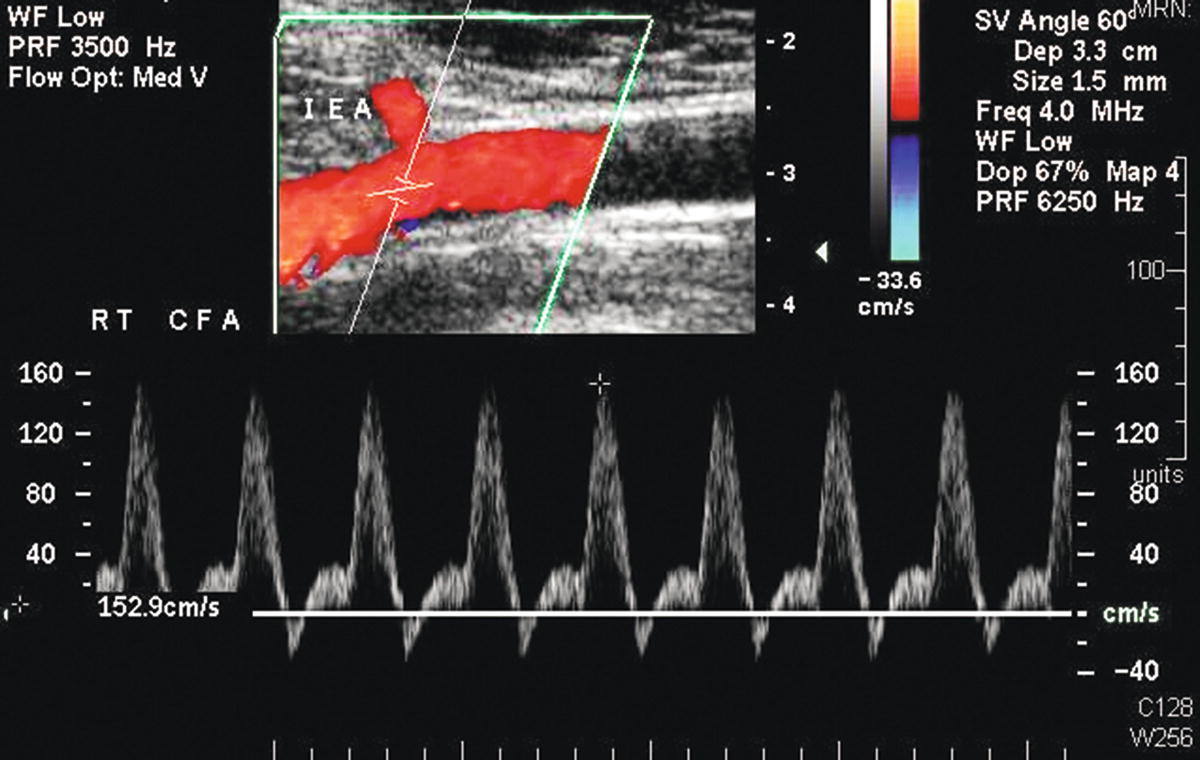
FIGURE 36.4. Color-flow image and Doppler spectral waveform from a common femoral artery (CFA) showing the origin of the deep inferior epigastric artery (IEA).
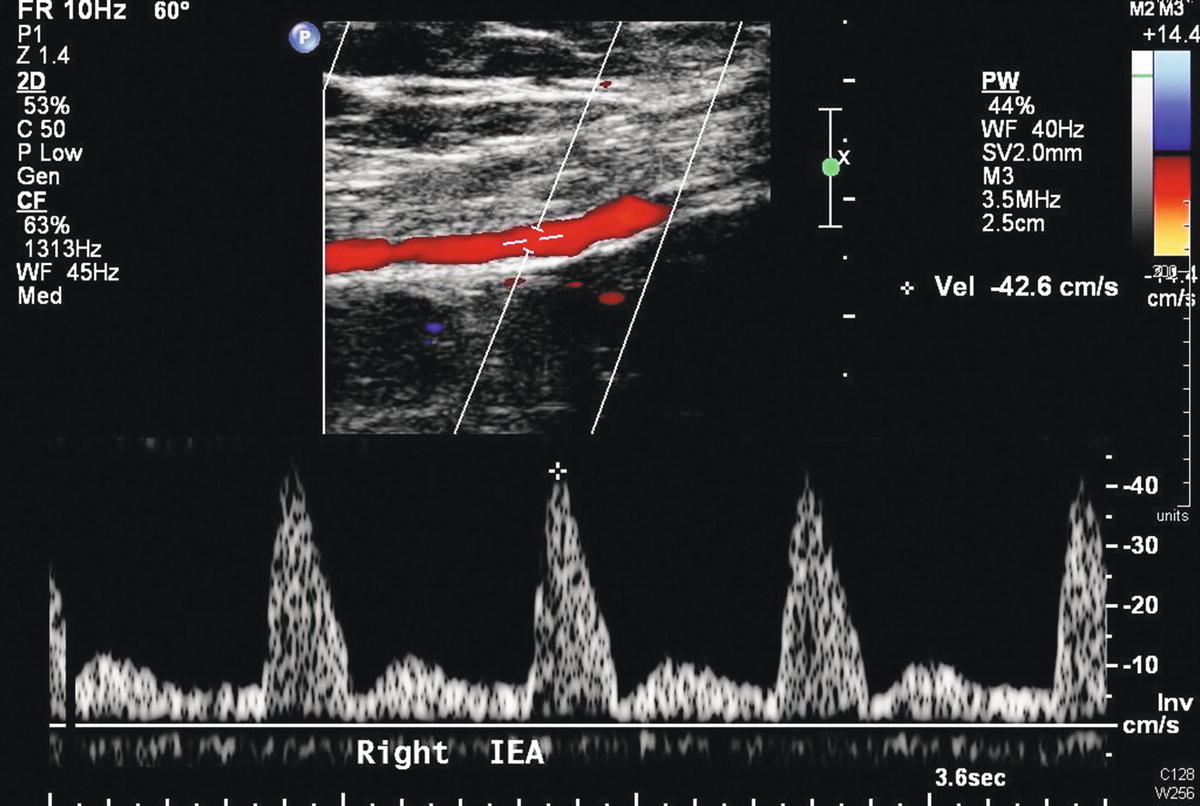
FIGURE 36.5. Duplex evaluation of the deep inferior epigastric artery (red) as it courses deep to the rectus abdominis muscle. The inferior epigastric artery (IEA) spectral waveform is also shown with a peak systolic velocity of about 43 cm/s.
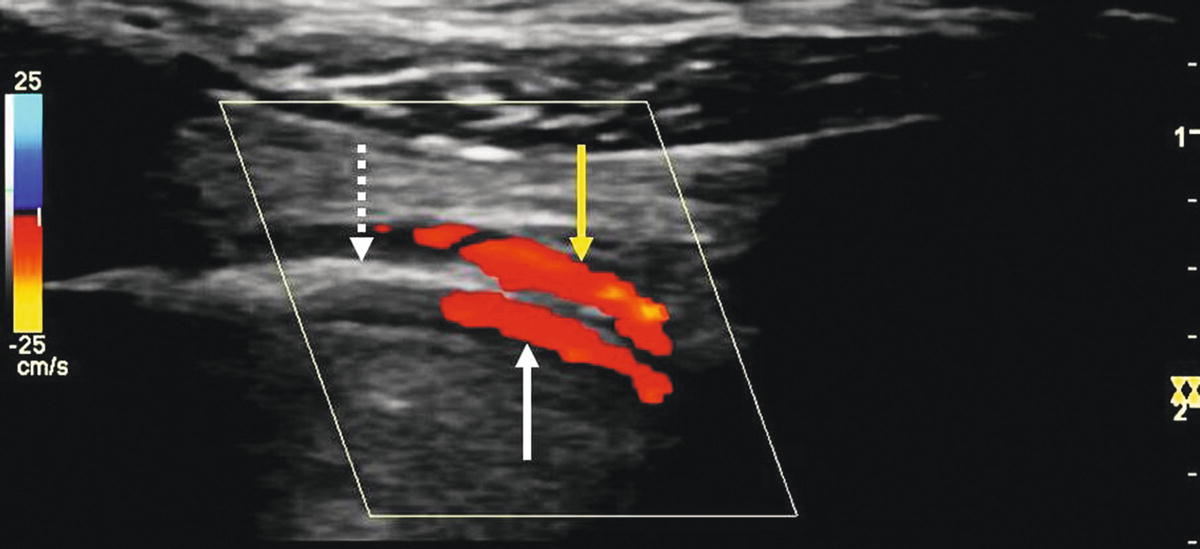
FIGURE 36.6. Duplex evaluation of the internal mammary artery. Ultrasound reflections from the pleura of the lung (dashed arrow) can create a mirror-image artifact that appears as two internal mammary arteries (solid arrows), one on each side of the pleura. The real internal mammary artery is on top (yellow arrow).
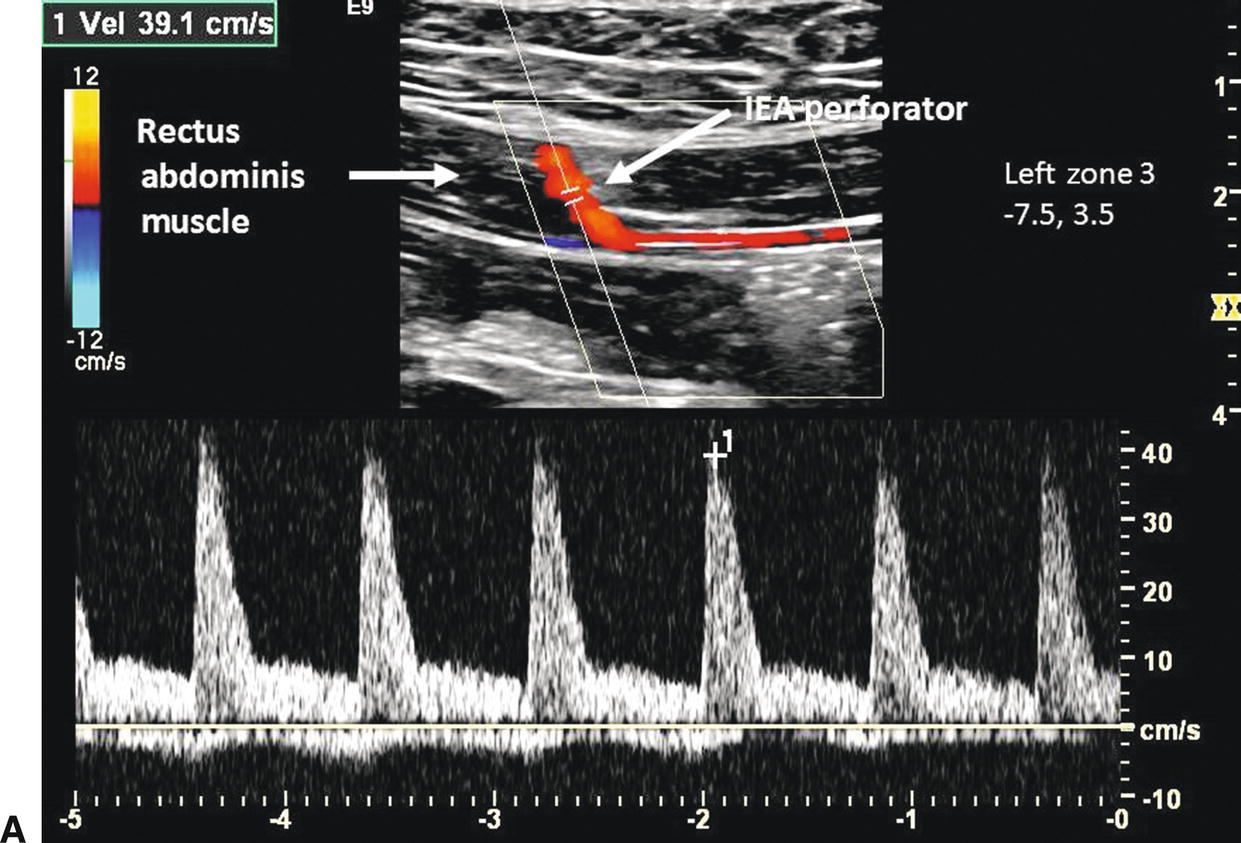
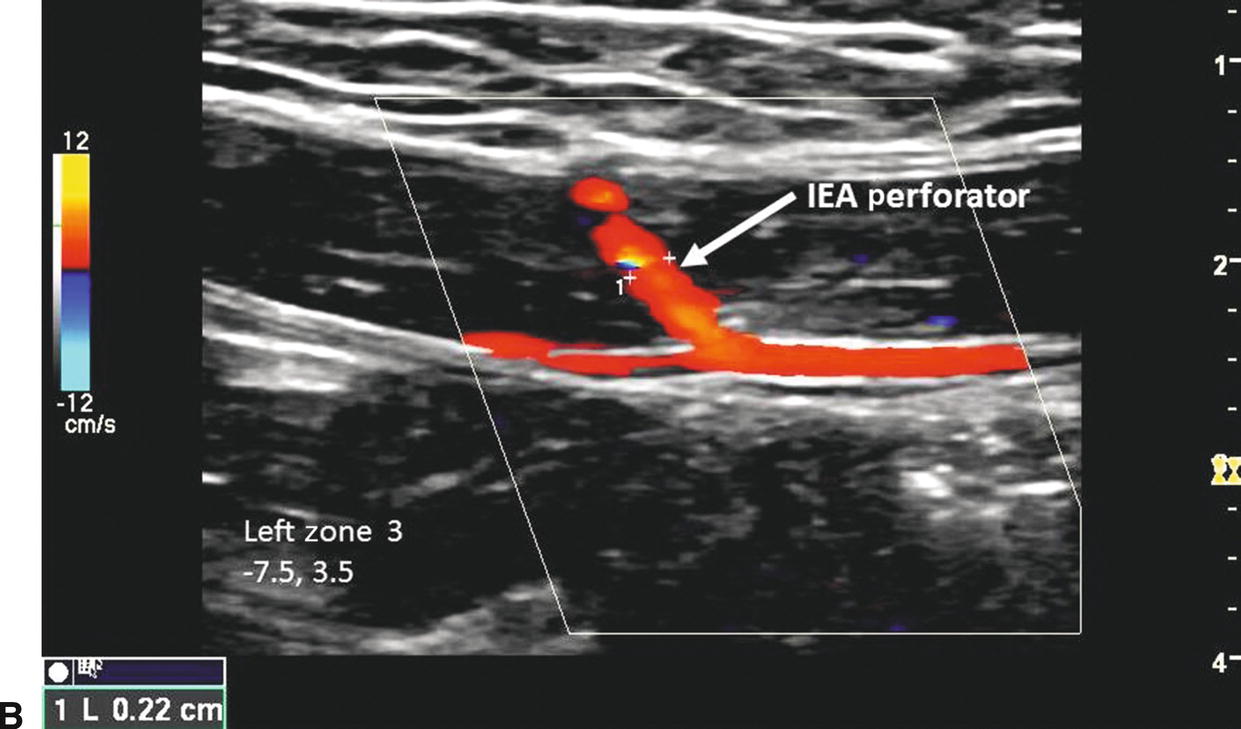
FIGURE 36.7. A,Peak systolic velocity measurement of 39 cm/s from an inferior epigastric artery (IEA) perforator in zone III on the left side. The perforator is located 7.5 cm below the umbilicus and 3.5 cm to the left of the midline. B,Diameter measurement of the same IEA perforator (0.22 cm).
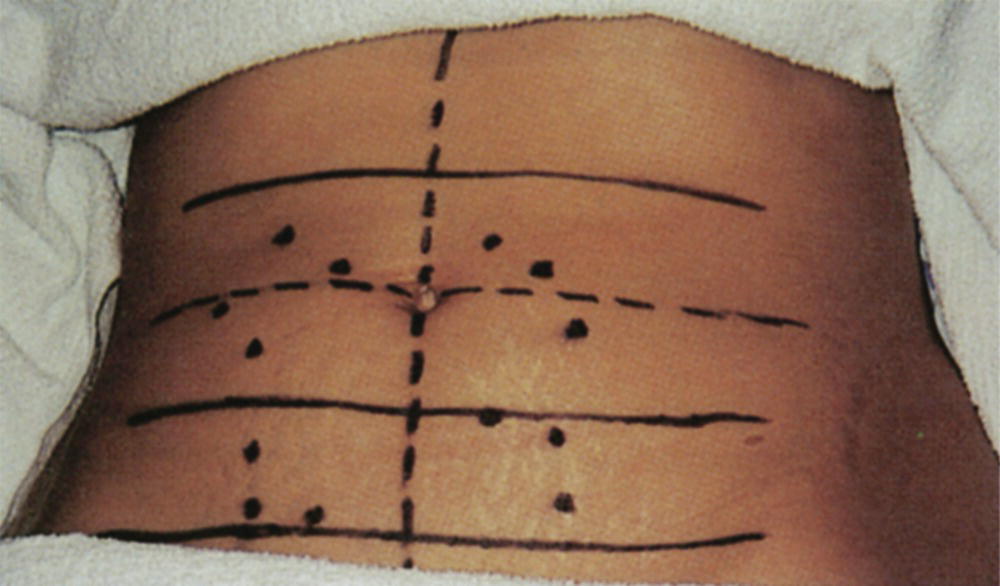
FIGURE 36.8. Markings from a preoperative TRAM flap duplex study show perforator locations on both sides for zones I, II, and III (zone IV not shown).
They concluded that the preoperative duplex examination allows the surgeon to incorporate a greater number of perforators into the flap and provides reliable information to identify any abnormal or unusual anatomy. The approach described by Cramer et al7 has been the protocol at the University of Washington prior to flap procedures for breast reconstruction until recently when CTA has also been used to visualize and evaluate perforator vessels.8
VASCULAR EVALUATION PRIOR TO FLAP SURGERY
The duplex evaluation performed in the vascular laboratory prior to flap procedures for breast reconstruction can be divided into three parts. First, patency of the inflow vessels to the perforator arteries of the rectus abdominis muscle must be documented. Second, the perforator arteries are assessed for flow (peak systolic velocity), size (diameter), and number. The locations of the perforator arteries are also marked on the skin preoperatively. Third, patency of the internal mammary, subclavian, and axillary arteries is documented. Depending on the type of surgical procedure to be done, one of these arteries may become the sole source of perfusion to the flap.
Evaluate Inflow to the Flap Tissue
The inflow vessel to the perforator arteries of the rectus abdominis muscle is the deep inferior epigastric artery, which originates from the distal external iliac or proximal common femoral artery. The iliac and common femoral arteries are evaluated by duplex scanning, using the B-mode image to locate the vessels and pulsed Doppler waveforms to document the peak systolic velocities and flow patterns. The velocity criteria for lower extremity arteries established by Jager et al9 are applied. A normal external iliac or common femoral artery is characterized by a triphasic flow pattern and uniform peak systolic flow velocities in the range of 80 to 120 cm/s. The normal deep inferior epigastric artery peak systolic velocities were noted by Cramer et al7 to range from approximately 40 to 45 cm/s. Stenosis is suspected if there is a focal velocity increase followed by a turbulent, poststenotic flow pattern. Lower extremity arterial duplex scanning is discussed in detail in Chapter 12.
Evaluate the Perforator Arteries
In 1994, Rand et al10 published their experience with 32 consecutive patients undergoing TRAM flap surgery and reported nearly 98% complete flap survival. One patient with a significant smoking history had a failed unilateral flap owing to venous occlusion. The preference in this series was to incorporate a minimum of three perforators with flow velocities greater than 20 cm/s into the flap. If the velocities were lower than 20 cm/s in three perforators, an effort was made to include additional perforators into the flap. One false-positive duplex assessment was reported in this study, but there were no false negatives.
Further validation for the role of duplex scanning prior to TRAM flap surgery was reported by Meunier et al.11 In this study, 20 patients were evaluated preoperatively using the protocol described by Rand et al.9 Four patients were rejected for the flap procedure after the duplex examination revealed an insufficient number of perforator arteries or perforator arteries that were small with low flow; the remaining 16 patients were considered candidates for surgery. These authors found two false negatives intraoperatively, and there were no false positives. Flap survival without revision was approximately 90%. This study did reveal two limitations of duplex scanning prior to flap procedures. First, the venous network of the muscle could not be evaluated, and venous congestion is one of the causes of complications after free flap surgery.12 Second, obesity (with increased depth of vessels) and abdominal scar tissue may interfere with ultrasound imaging.8
The clinical experience described previously and a study in cadavers by Heitmann et al13 provide a range of measurements and other parameters that can serve as guidelines. Any findings that fall outside these measurements should be brought to the attention of the surgeon. Table 36.2 lists the expected number of perforators per side and zone on the abdomen, and Table 36.3 gives the range of flow velocities normally found in the perforator and deep inferior epigastric arteries. Meunier et al11 reported average diameters for the deep inferior epigastric and perforator arteries. These diameter measurements are compared with the cadaver study performed by Heitmann et al13 in Table 36.4. According to Rand et al,10 the absence of at least one perforator per zone measuring a minimum of 1 mm, velocities of less than 13 cm/s in a perforator artery, or velocities of less than 40 cm/s in the deep inferior epigastric artery should be brought to the attention of the surgeon.
TABLE 36.2 Average Number of Rectus Abdominis Muscle Arterial Perforators Per Side and Per Zone

From Cramer MM, Rand RP, Strandness DE. Color flow duplex scanning: A technique to improve transverse rectus abdominis myocutaneous (TRAM) viability. J Vasc Technol 1993;17:7–16, with permission.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


