(1)
Department of General surgery, Fuwai Hospital, Beijing, China
28.1 General Considerations
DOLV is a rare deformity of the connection of the LV and the main artery. The two groups of main arteries both have origins from a morphological LV, generally accompanied by a VSD, usually the type under the AV.
The embryological theory is that the cause has something to do with abnormal absorption of the cone or another deformity such as pulmonary stenosis. The DOLV should be distinguished from the TGA in embryology, because both the AV and the PV originate from morphological LV. There is no fibrous connection of the two groups of main arteries and the MV, but there is fibrous connection of the AV, the PV, and the MV.
In this case, the DOLV is accompanied by a VSD under the AV and pulmonary stenosis, atrium and ventricle normotopia, a remaining muscular conical structure, a normal TV, and a small LV. Another case is ventricle inversus viscerum, DOLV. Surgical therapy is palliative operation or radical operation, according to the PAH or PS and the growth of the left and right ventricles (Fig. 28.1m).
28.2 Specimen Demonstrations
28.2.1 DOLV, Ventricle Normotopia
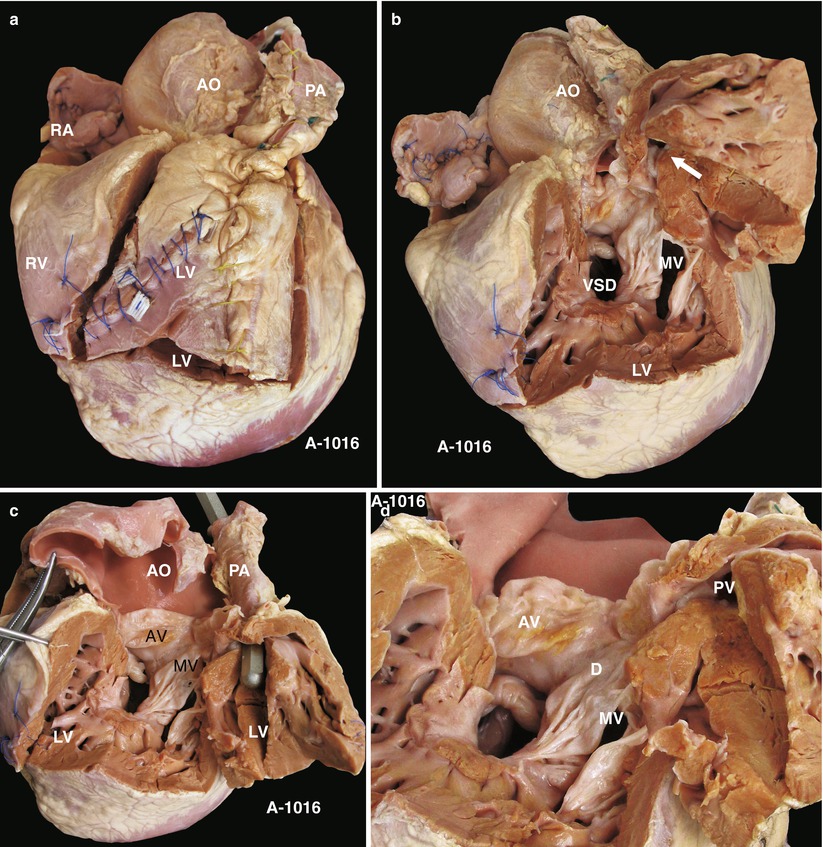
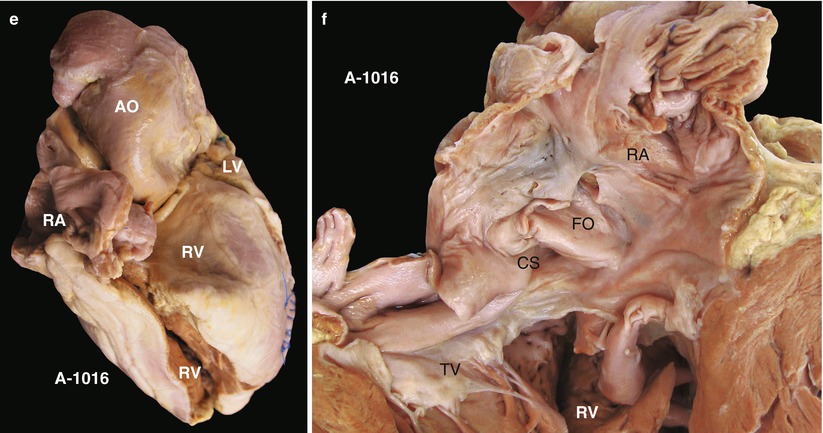
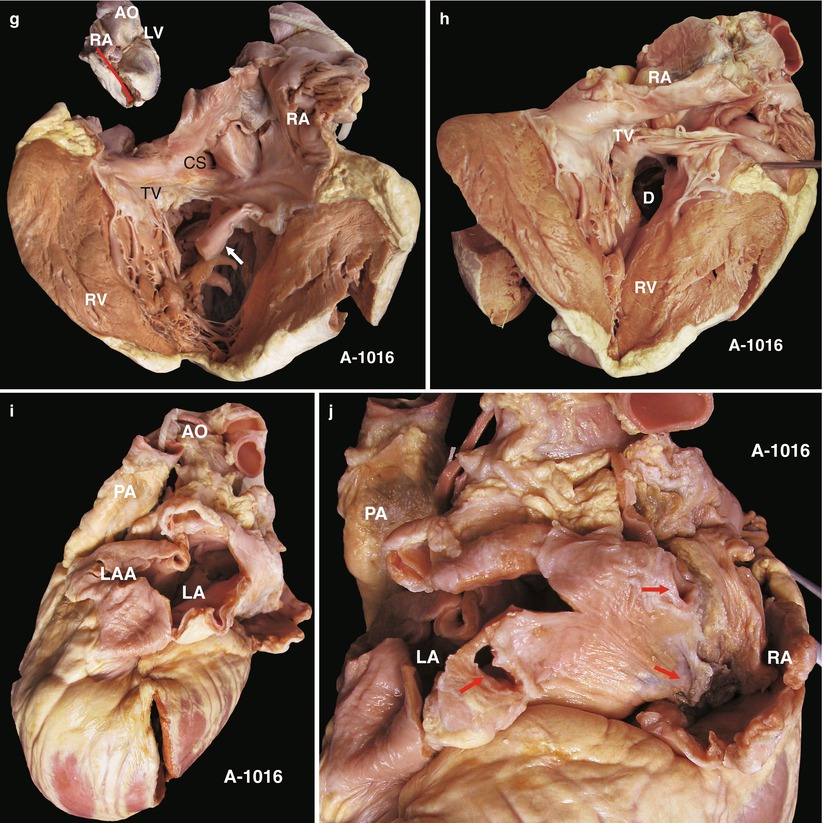
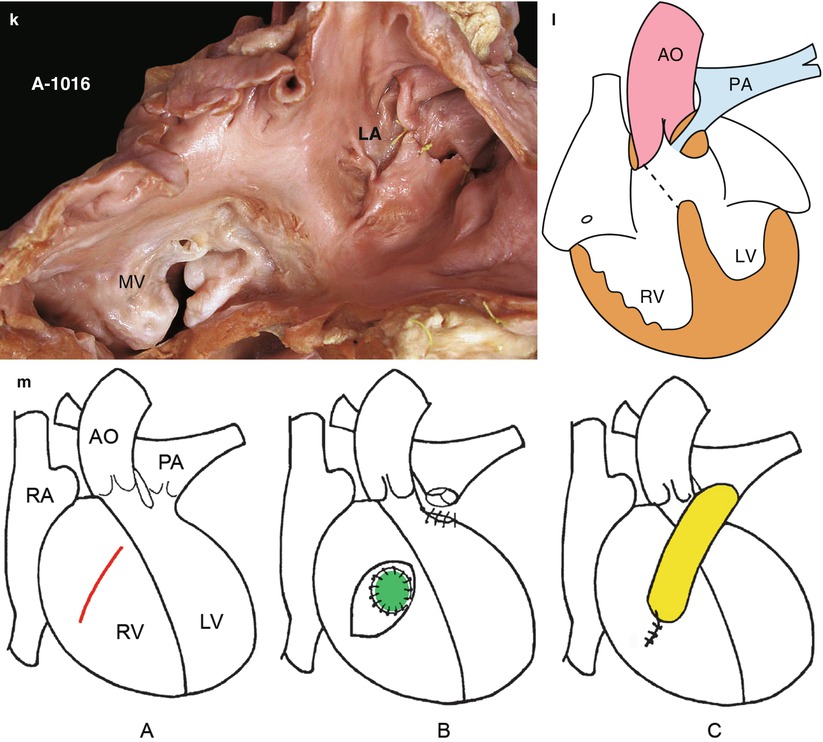
Fig. 28.1
(a) Specimen 1016. DOLV accompanied with muscular stenosis under pulmonary valve, rare in comparison. The anterior wall (dissociate wall) of the LV is straight ahead, the incision can be seen, and the main pulmonary artery is front and left of the aorta. PA pulmonary artery, AO ascending aorta, RA right atrium, RV right ventricle. (b) Specimen 1016. The dissociate wall of the LV, opened. Figure shows first, the diameter of the VSD is similar to the PV but much smaller than the AV; second, there is crack in the MV, and chordae tendineae of the anterior leaflet adhere to the edge of the VSD; third, there is a fibrous connection of the mitral, atrial, and pulmonary valves; fourth, the LV is small, and the enlarged RV is behind it; and fifth, the PV grows well, and there is mild pulmonary stenosis and a thick conical muscle under the pulmonary valve, which leads to obstruction under pulmonary artery (arrow). MV mitral valve. (c) Specimen 1016. The probe is inserted into the pulmonary artery, which reveals that both the pulmonary and aortic valves originate from the LV. There is fibrous connection of the mitral and aortic valves, and muscular pachynsis is present under PV. The LV is small, and chordae tendineae of the MV bestride on the VSD. PA pulmonary artery, AO ascending aorta. (d) Specimen 1016. Figure reveals the aortic, pulmonary, and mitral valves and the VSD (D) at close range. AV aortic valve, PV pulmonary valve, MV mitral valve. (e) Specimen 1016. From the right view. The right atrium and ventricle are divided at the same time, the aorta expands, the RV enlarges, and the main pulmonary artery is covered. LV left ventricle, AO ascending aorta, RA right atrium. (f) Specimen 1016. Figure reveals the coronary sinus and FO in the RA, which demonstrate a morphological RA. This clearly is atrium normotopia, in which the RA is on the right and the TV is normal. CS coronary sinus, RV right ventricle. (g) Specimen 1016. The right atrium and tricuspid valve viewed from the same angle as Fig. 28.1f. The arrow points to the anterior papillary muscle; there is no RVOT, rather a VSD. RA right atrium, CS coronary sinus, TV tricuspid valve, RV right ventricle. (h) Specimen 1016. A VSD observed in the right ventricle. There is no outflow tract or fibrous connection of the mitral and tricuspid valves, meaning there is no conjunction with the atrioventricular valve. Absence of an atrioventricular channel can be denied because the TV is normal. RA right atrium, RV right ventricle, D ventricular septal defect. (i) Specimen 1016. View of the left side of the heart. The main pulmonary artery grows well and is in the front and left of the aorta; the left atrium and auricle are enlarged. PA pulmonary artery, AO ascending aorta, LA left atrium, LAA left atrium auricle. (j) Specimen 1016. Figure shows that the doorway of the pulmonary vein is in the back (arrow), which proves the left side of the back wall is a morphological LA, another proof of atrium normotopia. PA pulmonary artery, RA right atrium. (k) Specimen 1016. Mitral valve in the left atrium. Thick leaflets, abnormal chordae tendineae, and papillary muscle can be seen. The chordae tendineae of the anterior leaflet adhere to the inferior border of the VSD; the “crack” could be considered as the crack of the anterior junction. LA left atrium, MV mitral valve. (l) Specimen 1016. Sketch map of the DOLV. The aorta and pulmonary artery both originate from the LV. The LV dysplasia is present: the diameter of the pulmonary artery is thinner than the aorta, and there is muscular conical stenosis under the PV, forming a VSD (dotted line). PA pulmonary artery, AO ascending aorta, RV right ventricle
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


