Diseases of the trachea can result in stenosis, malacia (softening of the trachea), and tracheomegaly and involve congenital, infectious, and neoplastic processes (Table 34.1). Neoplastic entities will be discussed later in the book.
Conditions that Result in Stenosis
Congenital Stenosis
Tracheal stenosis in infants is rare. There may be generalized hypoplasia, funnel-shaped narrowing tapering to stenosis just proximal to the carina, or segmental stenosis. Severe tracheal stenosis resulting in atresia occurs in two in 100,000 newborns and requires a tracheoesophageal fistula for spontaneous breathing.1
More than half of the infants who manifest clinical symptoms show a long-segment stenosis, most commonly caused by complete tracheal rings producing a “napkin-ring” stenosis.2 Vascular rings caused by congenital aortic arch anomalies and bronchogenic cysts may result in extrinsic compression of the trachea. Tracheal stenosis is more prevalent in infants with Down syndrome and may be associated with bronchial abnormalities and pulmonary agenesis.3
When limited in length, tracheal stenosis is amenable to resection with anastomosis. A variety of surgical options have been recommended.4
Relapsing Polychondritis
Relapsing polychondritis is an autoimmune disorder characterized by recurrent progressive inflammatory episodes involving cartilage of the ear, nose, larynx, peripheral joints, and tracheobronchial tree. In addition to stenosis, tracheomalacia can also occur. The disease generally presents in young adulthood. Respiratory tract involvement occurs in up to 50% of patients, is uncommon at presentation, and carries a poor prognosis. The larynx and subglottic trachea are most involved initially, with progression to the distal trachea and bronchi, often with patchy involvement.
Histopathologically, the disease is characterized by mixed acute and chronic inflammation in and around the cartilage. Tracheal stenosis occurs when there is fibrosis and contraction of the airway and may be severe. Loss of structural cartilaginous support may result in tracheobronchomalacia. The process is centered on the cartilage and therefore spares the posterior membranous wall of the trachea, unless there is constrictive fibrosis.5,6
Severe stenosis may necessitate tracheostomy in addition to steroid therapy. Stenting to the level of the tracheal bifurcation may also be required.7
Amyloidosis
Pulmonary amyloidosis occurs in three forms (see Chapter 27): diffuse interstitial amyloidosis, nodular amyloidosis, and tracheobronchial deposits of submucosal amyloid. Tracheobronchial amyloidosis occurs in only 1.1% of patients with amyloid.8 Computed tomography demonstrates nodular and irregular narrowing of the tracheal lumen. Pulmonary manifestations include lobar or segmental collapse, recurrent pneumonia, bronchiectasis, and obstructive hyperinflation.8 There may be secondary mural calcification or ossification of the lesions, leading to confusion with tracheobronchopathia osteochondroplastica, although there is no sparing of the posterior membrane.
Sarcoidosis
Although distal bronchial involvement is common in sarcoidosis, the larynx and upper trachea are affected in only in 1% to 3% of patients, with a slightly higher rate of involvement of the distal trachea and mainstem bronchi. Narrowing of the airway is caused by extrinsic compression by paratracheal lymph nodes or may be the result of thickening of the mucosa and submucosa by sarcoid granulomas. The classic endobronchial finding is the raised “cobblestone” appearance of the mucosa.5 Positive biopsies show granulomas, typically nonnecrotizing, in the lamina propria or submucosa (see Chapter 22).
Granulomatosis with Polyangiitis
Airway involvement is found in 15% to 55% of patients with granulomatosis with polyangiitis (GPA, Wegener granulomatosis) (see Chapter 48) and is more frequent in women younger than 30 years.9 More distal thickening in the segmental and subsegmental bronchi is present in almost 75% of patients.10 Subglottic stenosis is the most frequent airway manifestation in GPA, seen in 9 of 10 patients in one series.10
TABLE 34.1 Diseases Affecting the Trachea and Proximal Bronchi
Conditions that result in tracheobronchial narrowing
Congenital stenosis
Relapsing polychondritis
Amyloidosis
Sarcoidosis
Systemic autoimmune diseases
• Wegener granulomatosis
• Ulcerative colitis
Tracheopathia osteoplastica
IgG4-related disease
Postintubation
Tracheobronchomalacia
Congenital
COPD
Trauma
Cystic fibrosis
Polychondritis
Tracheobronchomegaly (Mounier-Kuhn disease)
Miscellaneous congenital conditions
Tracheal bronchus
Accessory cardiac bronchus
Congenital bronchial atresia
Infections
Viral
Fungal
Bacterial
Benign tumors
Solitary papillomas
Recurrent respiratory papillomatosis
Hamartomas
Granular cell tumor
Malignant tumors
Squamous cell carcinoma
Adenoid cystic carcinoma
Metastatic tumors
• Local extension: thyroid, esophagus, larynx, lung
• Hematogenous: melanoma, renal cell, breast
Histopathologically, endobronchial biopsies of tracheobronchial GPA show necrosis, giant cells, vasculitis, capillaritis, and microabscesses. Slightly more than one-third of biopsies show features supportive of the diagnosis, whereas the remainder show nonspecific inflammation or are normal.9
Inflammatory Bowel Disease
Tracheobronchial involvement of Crohn disease is rare and can manifest as airway obstruction, including luminal narrowing from the subglottic trachea to the proximal main bronchus.11 Large airway involvement may also complicate ulcerative colitis, as diffuse sclerosing tracheobronchitis.12 Histologic features are nonspecific and show acute and chronic tracheitis with mucosal ulceration, diffuse and chronic submucosal inflammation, and fibrosis.
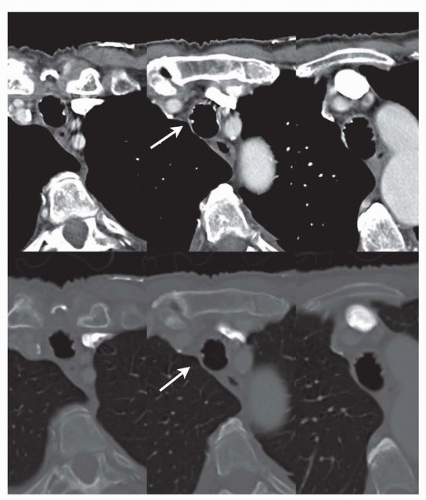
Tracheobronchopathia osteochondroplastica is an idiopathic disease of the trachea and large bronchi characterized by submucosal fibro-osseous nodules projecting into the lumens of the airways. Only 0.1% of all endobronchial biopsies show features consistent with the disease.13 Patients are usually elderly and generally asymptomatic but may complain of nonproductive cough and dyspnea. By computed tomography, small submucosal osteocartilaginous nodules of high density consistent with calcium are present in the cartilaginous portion of the airways sparing the posterior portion (Fig. 34.1).
FIGURE 34.1 ▲ Tracheobronchopathia osteochondroplastica. CT scan shows projections into the tracheal lumen (arrows) some of which are of bone density. The anterior distribution and sparing of the posterior membranous trachea are evident.
Endobronchial or endotracheal biopsy is diagnostic in 70% of patients with the disease but frequently requires multiple biopsies, because the bony lesions are difficult to grasp with the bioptome.14 Autopsy studies have shown osseous and cartilaginous nodules in the tracheal submucosa and lamina propria. Serial sections of the nodules have demonstrated continuity between the submucosal lesions and the tracheal cartilaginous rings only a minority of cases. Squamous metaplasia is common in the overlying mucosa.14
The differential diagnosis includes relapsing polychondritis and tracheobronchial amyloidosis. If dystrophic ossification or chondroid metaplasia involving the submucosa or lamina propria is found, the diagnosis of tracheobronchopathia osteochondroplastica can be assumed. Calcification of airway cartilage may be normal in old age, particularly in women, but are not associated with soft tissue ossification. Similarly, relapsing polychondritis results in degeneration and secondary calcification of the cartilage, but block-like calcification and nodular calcifications of the lamina propria and submucosa are absent. Amyloidosis has been reported in a subset of patients with tracheobronchopathia osteochondroplastica; therefore, Congo red staining can be a useful adjunct.
Tracheobronchial Tuberculosis
Tuberculosis is in the differential diagnosis of diffuse tracheobronchial thickening. Tracheobronchial tuberculosis has been reported in 10% to 40% of patients with pulmonary parenchymal tuberculosis through bronchoscopic examination15 (see Chapter 40). In over half of patients, there are parenchymal lesions with paratracheal or peribronchial lymphadenopathy. In the remainder of the patients, a lack of parenchymal lesions suggests direct submucosal spread of mycobacterium along the peribronchial lymphatic channels. Sputum cytology has a relatively low yield, but high-resolution computed tomography is more sensitive in demonstrating tubercular involvement of tracheobronchial tree.
Endobronchial tuberculosis is more prevalent in young female patients. There is typically involvement of the long segment of the distal trachea and proximal bronchi. The endoscopic gross appearance has been classified as actively caseating, edematous-hyperemic, fibrostenotic, tumorous, granular, ulcerative, and bronchitic, with the granular and caseating types more likely to yield positive culture.16 The fibrostenotic type accounts for < 10% of cases. Fibrosis with luminal narrowing or obstruction is more frequent in the left main bronchus.5 Some degree of stenosis may develop in up to 90% of patients with endobronchial tuberculosis despite antimicrobial treatment. Imaging findings may occasionally mimic bronchogenic carcinoma, necessitating biopsy to for definitive diagnosis.5
Bronchoscopic biopsy is considered the most reliable method for confirmation of the diagnosis of endobronchial tuberculosis, with 30% to 84% sensitivity.15 Granulomatous inflammation (with or without necrosis) as well as necrosis without overt granulomatous inflammation are considered diagnostic. Other nonspecific findings include edema of the lamina propria, nodular fibrosis, and chronic bronchial inflammation with linear fibrosis.16
IgG4-Related Disease
Tracheobronchial stenosis is a rare manifestation of pulmonary IgG4-related disease.17 More commonly, bronchovascular bundles in the lung parenchyma are involved18,19 (Chapter 51). IgG4 disease may result in a mediastinal mass (sclerosing mediastinitis) that infiltrates the trachea20 and, occasionally, diffuse bronchial wall thickening.21 Airway involvement is typically but not invariably accompanied by bilateral hilar lymphadenopathy.22 Endobronchial or endotracheal biopsy may disclose features typical of IgG4-related disease, namely, storiform fibrosis, entrapment of veins and lymphoid tissue, and lymphocytic infiltrate with abundant IgG4-positive plasma cells (Fig. 34.2).
Only gold members can continue reading. Log In or Register to continue