After reading this chapter you will be able to: The purpose of mechanical ventilation is to support the patient until the disease state or condition that caused the need for support is alleviated or resolved.1–3 Ventilatory support can sustain life, but it cannot cure disease. Further, many complications and hazards are associated with mechanical ventilation. Consequently, ventilatory support should be withdrawn as soon as the patient is able to adequately resume spontaneous breathing.1–4 All patients who are mechanically ventilated should be evaluated on a daily basis for their ability to wean from ventilatory support.5,6 After the problem or condition that caused the need for mechanical ventilation is resolved, most patients can be quickly and easily removed from ventilatory support. For example, for most patients who need mechanical ventilation as a result of drug overdose or severe asthma, for those who are recovering from postoperative anesthesia, and for those who have received ventilation for 72 hours or less, one may simply discontinue ventilation when the precipitating condition has resolved.1,5 However, some patients require mechanical ventilation for longer periods. The term ventilator dependent is usually reserved for patients who need ventilatory support for lengthy periods (i.e., 2 weeks or more) or who have not responded to attempts at ventilator discontinuation.3 For these patients, a more formal ventilator discontinuation process is required.3 Ventilator discontinuation should be carefully timed.4 Premature removal from the ventilator may severely stress the cardiopulmonary system and delay the patient’s recovery.4 Premature discontinuation also exposes the patient to the hazards of reintubation. However, delays in discontinuing ventilation expose the patient to an increased risk of complications, including nosocomial pneumonia, myocardial infarction, and death.6 There are three basic methods for discontinuing ventilatory support: 1. Spontaneous breathing trials (SBTs) alternating with mechanical ventilation 2. Synchronized intermittent mandatory ventilation (SIMV) Other techniques that may facilitate ventilator discontinuation include the use of volume-support ventilation (VSV), adaptive support ventilation (ASV); automatic tube compensation (ATC); proportional assist ventilation (PAV), which is also known as proportional pressure support (PPS); and continuous positive airway pressure (CPAP).4,7–9 However, little data exist that support the use of any of these techniques except CPAP during the ventilator discontinuation process. Techniques for predicting when patients are ready for ventilator discontinuation and weaning have been studied extensively.6 Many weaning indices have been used, and a number of different weaning methods have been advocated. Despite this, there are no universally applicable rules for predicting success. Of all of the methods studied, SBTs and PSV have been shown to be the most effective methods for ventilator discontinuation and weaning. Evidence-based reviews recommend the use of at least daily SBTs.3 Protocols for ventilator discontinuation administered by an interdisciplinary team of respiratory therapists, nurses, and physicians can be highly effective, and the use of ventilator discontinuation protocols has also been recommended.3,6,10–13 Regardless of the method used, success is unlikely unless the precipitating problems that caused the ventilator dependency have been resolved.1,3,7,14 After these problems are resolved, an organized plan or protocol should be followed, and variations should be based on each patient’s response.3,6,10 Some patients cannot be successfully removed from mechanical ventilatory support. This group of ventilator-dependent patients poses clinical, economic, and ethical concerns.15 Many clinicians use the term weaning as a general term to refer to the process of discontinuing ventilatory support, regardless of the time frame or method involved.7,8,16 The term has also been used to refer to reductions in fractional inspired oxygen concentration (FiO2), PEEP, and CPAP.8 Alternatively, the term ventilator discontinuation has been used to refer to the process of disconnecting a patient from mechanical ventilatory support. For the purposes of this chapter, the term weaning is defined as a gradual reduction in the level of ventilatory support,1,7–9 whereas discontinuing ventilatory support refers to the overall process of removing the patient from the ventilator, regardless of the method used.3 In general, patients who are being considered for removal from ventilatory support fall into one of four categories: 1. Those for whom removal is quick and routine, which is normally the vast majority of ventilated patients 2. Those who need a more systematic approach to discontinuing ventilatory support, which is normally about 15% to 20% of ventilated patients 3. Those who require days to weeks to wean from ventilatory support, which is usually less than 5% of ventilated patients 4. Those ventilator-dependent or “unweanable” patients, who compose less than 1% of patients who require ventilatory support17 Patients may require mechanical ventilation because of apnea, acute or impending ventilatory failure, or severe oxygenation problems that necessitate high levels of PEEP or CPAP. Regardless of the reason for initiating mechanical ventilation, patients remain dependent on the ventilator because of respiratory, cardiovascular, neurologic, or psychologic factors.3 Patients who need mechanical ventilation often have a ventilatory workload or demand that exceeds their ventilatory capacity. This is the most common cause of ventilator dependence.1,2 The term ventilatory workload refers to the amount of work that the respiratory muscles are asked to perform to provide an appropriate level of ventilation. A patient’s total ventilatory workload is primarily determined by the following: (1) the level of ventilation needed; (2) the compliance of the lungs and thorax; (3) the resistance to gas flow through the airways, and (4) any imposed work of breathing (WOBi) due to mechanical factors.1,7 Mechanical factors that can increase the work of breathing include artificial airways (i.e., endotracheal and tracheotomy tubes), partial obstruction of the airway, ventilator circuits, demand flow systems, auto-PEEP, and inappropriate ventilator flow and sensitivity settings. Factors that may increase ventilatory workload are summarized in Box 47-1. Ventilatory capacity is determined by CNS drive, ventilatory muscle strength, and ventilatory muscle endurance.18 Most patients who are being withdrawn from ventilatory support have a normal or an increased drive to breathe. Patients with neuromuscular disorders and those who are receiving sedatives, narcotics, or neuromuscular blocking agents may have a reduced drive to breathe or impaired neuromuscular transmission. Patients with metabolic alkalosis, hypothyroidism, and sleep deprivation also may have reduced ventilatory drive. Box 47-2 summarizes the factors that may reduce ventilatory drive. Muscle strength is influenced by age, sex, muscle bulk, and overall health. Malnutrition, starvation, and electrolyte imbalances (especially involving calcium, magnesium, potassium, and phosphate) can lead to ventilatory muscle weakness.18,19 Critical illness myopathy, critical illness polyneuropathy, and the prolonged use of neuromuscular blocking agents are major causes of the development of ventilatory muscle weakness in the intensive care unit (ICU).20 Controlled ventilation for prolonged periods can result in ventilatory muscle discoordination and atrophy.18 Ventilatory muscle endurance is a function of energy supply versus demand. Energy supply is related to nutrition, perfusion, and cell use, whereas demand is related to the amount of work performed and is a function of minute ventilation, compliance, and resistance. Figure 47-1 summarizes the relationship between ventilatory demands and capabilities. Success with the discontinuation of ventilatory support is related to the patient’s condition in four main areas1,2,7: Simply put, when ventilatory workload or demand exceeds ventilatory capacity, successful ventilator discontinuation is unlikely.1,2 Excessive ventilatory workload may lead to ventilatory muscle fatigue. When the ventilatory muscles fatigue, they must be rested for at least 24 hours to recover.3,4,19 Ventilatory workload increases with decreased compliance, increased airway resistance, or an increased level of ventilation. Ventilatory capacity can be reduced by ventilatory muscle fatigue and by a loss of muscle strength and endurance. Other factors that may contribute to ventilator dependence include inadequate arterial oxygenation, poor tissue oxygen delivery, myocardial ischemia, arrhythmias, low cardiac output, and cardiovascular instability.7,16 Neurologic problems that may contribute to ventilator dependence include decreased central drive to breathe and impaired peripheral nerve transmission.3 Psychologic issues that may contribute to ventilatory dependence include the fear of removal of the life support system, anxiety, stress, depression, and sleep deprivation.3 Box 47-3 summarizes the major factors that contribute to ventilator dependence. Box 47-3 Factors That Contribute to Ventilator Dependence • Ventilatory workload exceeds ventilatory capacity • Decreased compliance: lung or chest wall • Increased resistance: artificial airways, bronchospasm, mucosal edema, secretions, and mechanical demand flow systems • Increased dead space: pulmonary embolus and COPD • Ventilatory muscle weakness or fatigue Data from MacIntyre N: Respiratory factors in weaning from mechanical ventilatory support. Respir Care 40:244, 1995; Slutsky AS: Mechanical ventilation. American College of Chest Physicians’ Consensus Conference. Chest 104:1833–1859, 1993; Pierson DJ: Nonrespiratory aspects of weaning from mechanical ventilation. Respir Care 40:263–270, 1995; MacIntyre NR, Cook DJ, Ely EW Jr, et al; American College of Chest Physicians; American Association for Respiratory Care; American College of Critical Care Medicine: Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest 120(6 Suppl):375S–395S, 2001. An important factor to consider as part of this assessment is the length of time that the patient has been receiving mechanical ventilation. In general, those who receive support for 72 hours or less often can be removed quickly from the ventilator.1,5,21 Those who need a longer period of support may need a more structured approach. Current guidelines recommend that patients who need mechanical ventilation for more than 48 to 72 hours be carefully assessed to determine all of the possible causes of ventilator dependence.3 These include the respiratory, cardiovascular, neurologic, and psychologic causes of ventilator dependence that are listed in Box 47-3. This recommendation is especially important for the care of patients who have had unsuccessful attempts at the discontinuation of ventilation.3 Factors associated with readiness for the discontinuation of ventilatory support are summarized in Box 47-4. The single most important criterion to consider when evaluating a patient for ventilator discontinuation or weaning is whether there has been significant alleviation or reversal of the disease state or condition that necessitated use of the ventilator in the first place.3,7,14 The clinician should determine whether the patient’s condition is improving, whether the initial reason for providing ventilatory support is improved or resolved, and whether the patient’s clinical condition is stable. The following specific questions for patient evaluation have been suggested3: 1. Is there evidence of improvement or reversal of the disease state or condition that caused the need for mechanical ventilation? 2. Is the patient’s oxygenation status adequate? Specific criteria may include the following: partial pressure of oxygen in the arteries PaO2 of 60 mm Hg or more, FiO2 of less than 0.40 to 0.50, PEEP of less than 5 to 8 cm H2O; PaO2/FiO2 of 150 to 200 or more; and pH of 7.25 or more. 3. Is the patient medically and hemodynamically stable? Specific criteria may include the absence of acute myocardial ischemia or marked hypotension. Patients should have adequate blood pressure without vasopressor therapy or with only low-dose vasopressor therapy (i.e., less than 5 µg/kg/min of dopamine or dobutamine). 4. Can the patient breathe spontaneously? The patient must be able to breathe spontaneously and have a sufficient drive to breathe if ventilator discontinuation is being considered. If the patient’s condition is improving, if the alleviation or reversal of the precipitating disease state or condition has occurred, if the patient is capable of spontaneous breathing, and if the oxygenation status and hemodynamic values are stable, then a formal evaluation for ventilator discontinuation should be performed.3 Mechanical ventilation is hazardous, and unnecessary delays in ventilator discontinuation increase the associated complication rate.3,4 Unfortunately, premature ventilator discontinuation may also cause serious problems, including difficulty with reestablishing the artificial airway and serious compromise of the patient’s clinical status.3,4 Clinical judgment has been found to be a poor guide to determining whether a patient is ready for ventilator discontinuation, and more specific indicators have been sought.4 Ideally, specific indicators or weaning indices would clearly show whether a patient is ready to have the ventilator removed and would help to avoid inappropriate ventilator discontinuation. Unfortunately, none of the current weaning indices are capable of predicting readiness for ventilator discontinuance with a high level of accuracy. Traditional discontinuation indices include the PaO2/FiO2 ratio, the alveolar-to-arterial partial pressure of oxygen difference [P(A–a)O2], the maximum inspiratory pressure (MIP), the vital capacity (VC), the spontaneous minute ventilation (VEsp), and the maximum voluntary ventilation (MVV).5,21 Newer indices include the rapid, shallow breathing index (f/Vt), airway occlusion pressure (P0.1), and measures of WOB.6–8 Although all of these values can be useful, there are enormous discrepancies in the literature regarding their accuracy with regard to the prediction of “weanability.”3,6,7 With respect to the more traditional discontinuation indices, vital capacity and MIP can be highly variable, whereas minute ventilation, respiratory rate (f), and f/Vt tend to be more reliable.22 However, these measures may not correlate well with discontinuation success among all patients and especially among those receiving long-term ventilatory support, the elderly, and those with major pulmonary abnormalities.5,18,23 A comprehensive evidence-based review identified a possible role for 66 specific measurements as predictors of weaning success.6 Of these, eight values were found to be the most useful for the prediction of successful ventilator discontinuation.3,6 Useful predictive measures included spontaneous respiratory rate, spontaneous tidal volume, f/Vt, minute ventilation, MIP, P0.1, P0.1/MIP, and a combined index called the CROP score that included compliance, rate, oxygenation, and MIP.3,6 Unfortunately, these measures all have limitations and relatively high false-positive predictions in specific settings. It is doubtful that a single index will be found that can be used for consistent discrimination between discontinuation success and failure.7 Moreover, none of these traditional indicators alone has proved useful for the prediction of improvements in patient outcome or in the selection of a particular discontinuation method.7,10 The likely explanation for this failure to identify any consistently powerful discontinuation predictor is that patients’ conditions vary greatly and, for research purposes, clinicians already fully consider information from predictors when choosing patients for trials of the reduction or discontinuation of ventilatory support.10,23 Notwithstanding these limitations, the measurement of discontinuation indices in the difficult-to-wean patient may provide guidance with regard to the reasons that patients fail discontinuation trials. Many find it useful to trend these data on a daily basis for those patients who require lengthy weaning times.15 Specific values for respiratory indices that are used to predict the successful discontinuation of ventilatory support are found in Table 47-1. TABLE 47-1 Indices That Are Used to Predict the Success of Weaning and Ventilator Discontinuation Data from MacIntyre NR, Cook DJ, Ely EW, et al: Evidence-based guidelines for weaning and discontinuing ventilator support: a collective task force facilitated by the American College of Chest Physicians, the American Association for Respiratory Care, and the American College of Critical Care Medicine. Chest 120:375S–395S, 2001; AHRQ publication no. 01-E010, Rockville, MD, 2000, Agency for Healthcare Research and Quality; American College of Chest Physicians: Chest 104:1833, 1993; Burns SM et al: Am J Crit Care 4:4, 1995; Sharar S: Resp Care 40:239, 1995; Bassili HR, Deitel M: JPEN J Parenter Enteral Nutr 5:161, 1981. Increased thoracic cage movement during spontaneous breathing and asynchronous chest-wall-to-diaphragm movement are related to an increased workload that may lead to ventilatory muscle fatigue and failure.19 Tachypnea (i.e., more than 30 to 35 breaths/min) is a sensitive marker of respiratory distress, but it can prolong intubation if it is used as an exclusive criterion.25 Irregular spontaneous breathing or periods of apnea indicate that the patient is at risk for weaning failure. Asynchronous and rapid, shallow breathing patterns—although not definitive—suggest respiratory decompensation.19 The evaluation of patients for the presence of palpable scalene muscle use during inspiration, an irregular ventilatory pattern, palpable abdominal muscle tensing during expiration, and the inability to alter the ventilatory pattern on command can be helpful for the assessment of the potential for prolonged spontaneous ventilation. Patients with none of these signs have a 90% chance of success.26 Patients with one or two of these signs usually need continued support. The presence of three or more of these signs can mean that the patient’s condition is unstable and that the patient has a poor prognosis for ventilator removal. P0.1 is the inspiratory pressure that is measured 100 milliseconds after airway occlusion.21 The P0.1 is effort independent, and it correlates well with central respiratory drive.19 Ventilator-dependent patients with COPD who have a P0.1 of more than 6 cm H2O tend to be difficult to wean.21 The f/Vt is the ratio of spontaneous breathing frequency (breaths/min) to tidal volume (liters), and it has been found to be a good predictor of discontinuation success for the care of many patients who need mechanical ventilation.4,6,23 The f/Vt has less predictive power for the care of patients who need ventilatory support for longer than 8 days, and it may be less useful for predicting discontinuation success among elderly patients.8,23,27 Adjusting the threshold value for f/Vt to 130 or less measured at 3 hours was very effective for predicting discontinuation success among patients 70 years old and older. Despite these limitations, an f/Vt of less than 105 can be an accurate and early predictor of weaning outcome, and an f/Vt of 80 is associated with an almost 95% probability of successful discontinuation.4,23 The ratio must be calculated during 1 minute of unsupported spontaneous breathing, and the addition of pressure support significantly reduces the predictive value of the ratio.4 The P0.1/MIP ratio has been found to be a good early predictor of discontinuation success,3,19 and it may be more useful than the MIP by itself. The f/Vt also has been found to be a better predictor of discontinuation success than the MIP alone.2,3 However, even with f/Vt of less than 105, as many as 20% of patients have false-positive results (i.e., they cannot be discontinued from ventilation despite a favorable index) as a result of unpredictable factors such as congestive heart failure, aspiration, or the development of a new pulmonary lesion.28 However, some patients can be successfully discontinued from ventilatory support despite poor f/Vt values.29 Mini Clini Calculating and Interpreting the Rapid, Shallow Breathing Index WOB would seem to be an excellent way to gauge spontaneous ventilatory workload. Successful weaning has been found to be less likely among patients with spontaneous WOB levels of more than 1.6 kg/m/min (16 J/min) or 0.14 kg/m/L (1.4 J/L).5 However, WOB may not be predictive of weaning success for specific patients.7 This may be because WOB does not take into account ventilatory muscle capacity or fatigue. Consequently, WOB may be less accurate than other conventional discontinuation indices, and it is very difficult to measure at the bedside.30 Both OCB and %VO2 have been correlated with the number of days required to wean patients.19 Patients with an OCB of 15% or less of the total VO2 may be more likely to achieve discontinuation success. In one study, OCB was a better predictor of discontinuation success than was f/Vt.31 Pressure–time product (i.e., the area under the inspiratory pressure–time curve) and pressure–time index (PTI) may be the best measures of ventilatory workload for the care of patients who are receiving mechanical support.1 The PTI can be calculated as follows: where MIP is maximum inspiratory pressure, Ti is the inspiratory time in seconds, and Ttot is the total respiratory cycle. The Ttot can be calculated by dividing 60 by the respiratory rate (f) (i.e., 60/f). A PTI of more than 0.15 to 0.18 has been associated with diaphragmatic fatigue,32 and a PTI of more than 0.15 cannot be sustained indefinitely.1 There is currently no well accepted and reliable way to measure ventilatory muscle fatigue for patients who are receiving mechanical ventilation.5 Poor oxygenation status is associated with weaning failure.3,7 Arterial blood gas (ABG) analysis, pulse oximetry, and continuous mixed venous oximetry have been used to monitor and assess the oxygenation status of patients before and during a discontinuation trial. In general, a PaO2 of more than 60 mm Hg (or of more than 55 mm Hg for patients with COPD with carbon dioxide retention) with an FiO2 of less than 0.40 to 0.50 and a PEEP of 5 to 8 cm H2O or less should be adequate for ventilator discontinuation.3,7 The PaO2/FiO2 ratio should be 150 to 200 mm Hg or more.3 With these values, a normal hemoglobin level, a normal oxygen saturation (SaO2), and adequate cardiac output and tissue perfusion are assumed. Specific indices used to assess oxygenation status are found in Table 47-1. Metabolic factors primarily affect discontinuation in those patients who require long-term ventilatory support. Although nutritional factors are important for all patients, they are unlikely to affect discontinuation in those who only require short-term ventilatory support. Nutrition should be adequate to maintain respiratory muscle mass and contractile force.16 Feeding should be adjusted according to individual patient needs; most patients need 1.5 to 2.0 times their resting energy expenditure.33 In addition, protein intake should be between 1 and 1.5 g/kg per day. Excessive carbohydrate feeding can increase carbon dioxide production and may precipitate acute hypercapnic respiratory failure.16 Parenteral nutrition solutions that contain amino acid formulations (e.g., arginine/lysine) can cause metabolic acidosis and thus increase ventilatory demand.33 Metabolic rate can increase as a result of fever or sepsis. Increased WOB, shivering, seizures, and agitation can also increase oxygen demand and should be evaluated. Adequate renal function is required to maintain acid–base homeostasis, electrolyte concentrations, and fluid balance.34 The patient ideally should have an adequate urine output (i.e., more than 1000 ml/day), and there should be no inappropriate weight gain or edema. Renal insufficiency can lead to metabolic acidosis, which increases respiratory drive. Electrolyte disorders can impair ventilatory muscle function.3,16 Key electrolytes should be normal (i.e., magnesium, 1.8 to 3 mEq/L; phosphate, 2.5 to 4.8 mEq/L; potassium, 3.5 to 5 mEq/L); see Chapter 16 for details. Fluid overload can lead to congestive heart failure and pulmonary edema, which may impair pulmonary gas exchange. Adequate cardiovascular function is needed to provide sufficient oxygen delivery to the tissues. Cardiac rate and rhythm and blood pressure should be evaluated.3,16 Tachycardia (i.e., a heart rate of more than 100 to 120 beats/min) and bradycardia (i.e., a heart rate of less than 60 to 70 beats/min) should be controlled. The presence of arrhythmias, hypotension (i.e., a blood pressure of less than 90/60 mm Hg), and severe hypertension (i.e., a blood pressure of more than 180/110 mm Hg) should be evaluated carefully before the discontinuation of ventilatory support is considered.3,19 Cardiac output and index measurements as well as central line and pulmonary arterial pressures (i.e., central venous pressure, pulmonary arterial pressure, and pulmonary capillary wedge pressure) may be helpful for the evaluation of cardiovascular function. Left ventricular dysfunction, myocardial ischemia, and cardiovascular instability are associated with decreased discontinuation success.3,21 Table 47-2 provides criteria for confirming cardiovascular stability. However, very few patients without primary cardiovascular dysfunction have pulmonary artery catheters in place. The assessment of cardiac output is usually by noninvasive means, and only arterial and central venous pressures are generally available. TABLE 47-2 Criteria for Confirming Cardiovascular Stability Adequate CNS function is needed to ensure stable ventilatory drive, adequate secretion clearance (i.e., coughing and deep breathing), and the protection of the airway (i.e., gag reflex and swallow). In addition, the level of consciousness, dyspnea, anxiety, depression, and motivation can affect discontinuation success.3,5 The patient ideally is awake and alert, free of seizures, and able to follow instructions.3,34 Patients should have an intact central drive to breathe and peripheral nerve function. Brainstem strokes, electrolyte disturbances, sedation, neuromuscular blocking agents, and narcotic drugs can impair the central neurologic control of ventilation.3 Mental status is a good predictor of discontinuation success, and patients who are not alert are at risk for upper airway obstruction, aspiration, and secretion retention. Obtunded patients should, at a minimum, have an adequate gag reflex and cough. Decreased levels of consciousness are associated with aspiration after extubation. The level of consciousness is affected by the use of narcotic, sedative, and analgesic drugs. Drugs with CNS depressant effects should be discontinued, if possible, before the withdrawal of ventilatory support and extubation.16 Protocols to reduce sedation and the daily cessation of sedative drugs may reduce weaning time12,35,36 (see the section on Spontaneous Awaking Trials). The use of neuromuscular blocking agents to allow for controlled ventilation should be avoided, because they may prolong mechanical ventilation.37 Psychologic factors may be among the most important nonrespiratory contributing factors that lead to ventilator dependence.3 Fear, anxiety, and stress should be minimized, and frequent communication among the staff, the patient, and the patient’s family can be helpful.3 Box 47-5 summarizes nonrespiratory factors that affect discontinuation success. Many factors are associated with discontinuation success. In an analysis of 217 patients, discontinuation success could be accurately predicted in about 75% of the patients when multiple predictors were combined.24 For all patients, regardless of diagnosis, days of mechanical ventilation (DMV), f/Vt; MIP, P0.1, maximum expiratory pressure, and VC—when used in combination—were the best predictors.24 For patients with acute respiratory failure, the best predictors were DMV, P0.1/MIP, MIP, f/Vt, and age (76.1% accurate); for patients with COPD, the best predictors were DMV, f/Vt, P0.1, P0.1/MIP, MIP, and age (93.9% accurate); and for patients with neuromuscular disease, MIP, maximum expiratory pressure, f/Vt, and P0.1 were the best predictors (73.9% accurate).24 Integrated indices improve prediction by combining several measures of ability to breathe without ventilatory support. Current examples of integrated indexes include the CROP score, the Adverse Factor/Ventilator Score, the weaning index, and the Burns Weaning Assessment Program.7,19 The CROP score combines measures of ventilatory load, respiratory muscle strength, and gas exchange.7,23 The Adverse Factor/Ventilator Score combines ratings of 15 adverse factors, including hemodynamic values, infection, nutrition, and neurologic/psychiatric state, with ratings of six ventilator factors, including FiO2, compliance, minute ventilation, and rate.19 The weaning index combines measures of ventilatory strength, endurance, and efficiency of gas exchange.19 A weaning index of less than 4 suggests successful discontinuation from mechanical ventilation.18,32 The Burns Weaning Assessment Program is a 26-item assessment that combines 12 general and 14 respiratory factors into a single score.19 Although integrated indices appear promising, no single index has emerged as superior for use in diverse patient populations. Despite the success of these integrated indices in very specific settings, the best approach to determining if a patient can be successfully discontinued from ventilatory support is the patient’s performance on spontaneous breathing trials. All patients should be assessed daily, and their ability to breathe spontaneously should be the primarily variable to determine if the ventilator can be discontinued.
Discontinuing Ventilatory Support
 Discuss the relationship between ventilatory demand and ventilatory capacity as well as their relationship with ventilator discontinuance.
Discuss the relationship between ventilatory demand and ventilatory capacity as well as their relationship with ventilator discontinuance.
 List the factors associated with ventilator dependence.
List the factors associated with ventilator dependence.
 Explain how to evaluate a patient before attempting ventilator discontinuation or weaning.
Explain how to evaluate a patient before attempting ventilator discontinuation or weaning.
 Contrast the advantages and disadvantages associated with various weaning methods and techniques.
Contrast the advantages and disadvantages associated with various weaning methods and techniques.
 Describe how to assess a patient for extubation.
Describe how to assess a patient for extubation.
 List the primary reasons why patients fail a ventilator discontinuance trial.
List the primary reasons why patients fail a ventilator discontinuance trial.
 Explain why some patients cannot be successfully weaned from ventilatory support.
Explain why some patients cannot be successfully weaned from ventilatory support.
Reasons for Ventilator Dependence
Ventilatory Workload or Demand
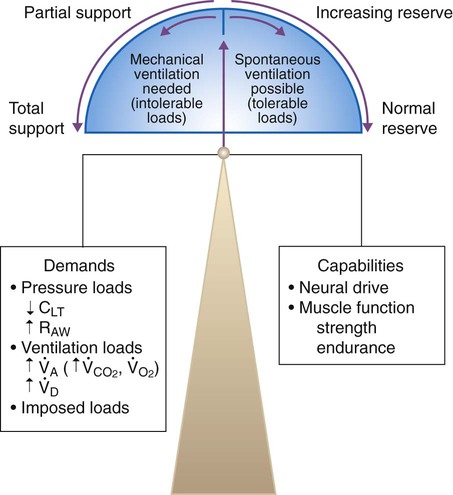
Ventilatory Capacity
Global Criteria for Discontinuing Ventilatory Support
Patient Evaluation
The Most Important Criterion
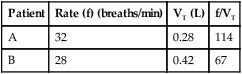
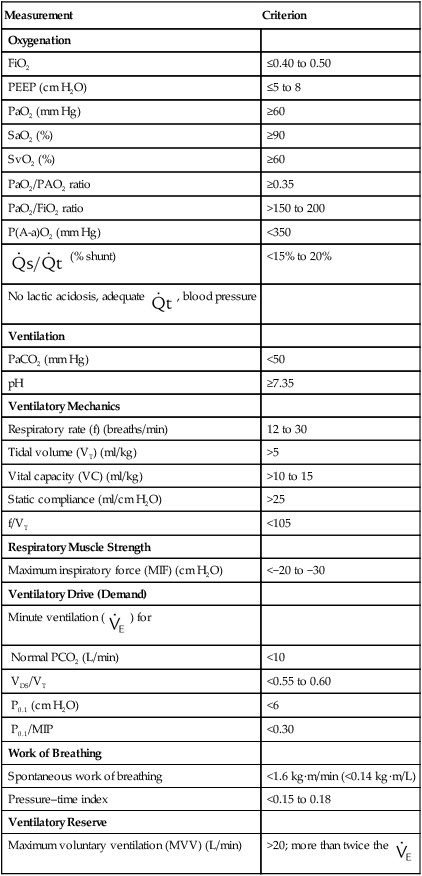
Weaning Indices
Measurement
Criterion
Oxygenation
FiO2
≤0.40 to 0.50
PEEP (cm H2O)
≤5 to 8
PaO2 (mm Hg)
≥60
SaO2 (%)
≥90
SvO2 (%)
≥60
PaO2/PAO2 ratio
≥0.35
PaO2/FiO2 ratio
>150 to 200
P(A-a)O2 (mm Hg)
<350
 (% shunt)
(% shunt)
<15% to 20%
No lactic acidosis, adequate  , blood pressure
, blood pressure
Ventilation
PaCO2 (mm Hg)
<50
pH
≥7.35
Ventilatory Mechanics
Respiratory rate (f) (breaths/min)
12 to 30
Tidal volume (VT) (ml/kg)
>5
Vital capacity (VC) (ml/kg)
>10 to 15
Static compliance (ml/cm H2O)
>25
f/VT
<105
Respiratory Muscle Strength
Maximum inspiratory force (MIF) (cm H2O)
<−20 to −30
Ventilatory Drive (Demand)
Minute ventilation (  ) for
) for
Normal PCO2 (L/min)
<10
VDS/VT
<0.55 to 0.60
P0.1 (cm H2O)
<6
P0.1/MIP
<0.30
Work of Breathing
Spontaneous work of breathing
<1.6 kg·m/min (<0.14 kg·m/L)
Pressure–time index
<0.15 to 0.18
Ventilatory Reserve
Maximum voluntary ventilation (MVV) (L/min)
>20; more than twice the 
Ventilation



Oxygenation
Metabolic Factors
Renal Function and Electrolytes
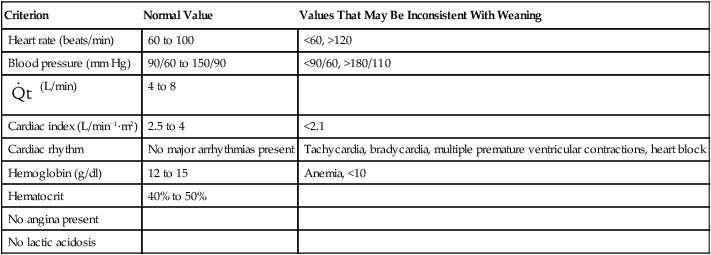
Cardiovascular Function
Criterion
Normal Value
Values That May Be Inconsistent With Weaning
Heart rate (beats/min)
60 to 100
<60, >120
Blood pressure (mm Hg)
90/60 to 150/90
<90/60, >180/110
 (L/min)
(L/min)
4 to 8
Cardiac index (L/min−1·m2)
2.5 to 4
<2.1
Cardiac rhythm
No major arrhythmias present
Tachycardia, bradycardia, multiple premature ventricular contractions, heart block
Hemoglobin (g/dl)
12 to 15
Anemia, <10
Hematocrit
40% to 50%
No angina present
No lactic acidosis
Psychologic Factors and Central Nervous System Assessment
Integrated Indices
Discontinuing Ventilatory Support



 , minute alveolar ventilation;
, minute alveolar ventilation;  , minute dead space ventilation.
, minute dead space ventilation. 

 Rule of Thumb
Rule of Thumb Problem
Problem