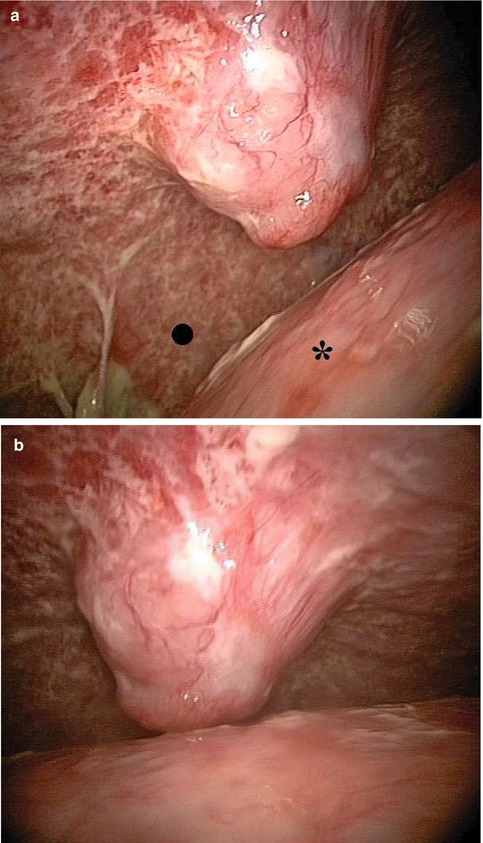
Fig. 10.1
Trapped lung (left lower lobe in this case – star) is not a contraindication to medical thoracoscopy in case with high clinical suspicion of neoplastic disease. In this case, a diagnosis of pleural adenocarcinoma was obtained after multiple biopsies of the posterior parietal pleura which had demonstrated non-specific white lymphangitis (⚪). Pleural fat is visible on the diaphragm (◻)

Fig. 10.2
Left side. Typical features of metastatic pleural effusion. Nodules are clearly visible on the posterior parietal pleura with hypertrophic lymphatic vessels (white bundles). The diaphragm is also invaded with nodules on the surface. After removal of the fluid, the costodiaphragmatic gutter will be carefully examined
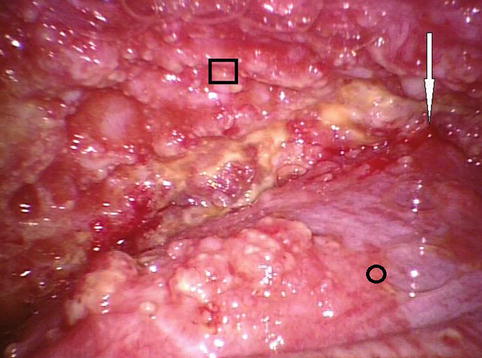
Fig. 10.3
Advanced malignant pleural effusion from a cancer of unknown origin. Disseminated pleural carcinomatosis is seen invading the posterior parietal pleura (◻) and the lung (⚪)
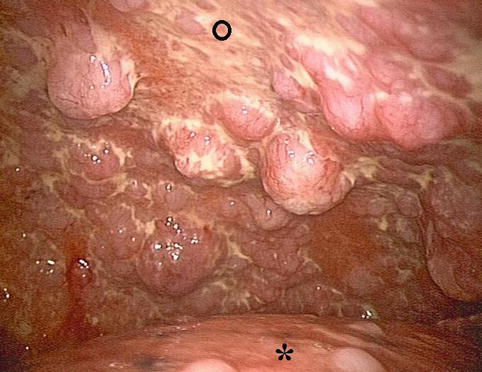
Fig. 10.4
Metastatic pleural cancer. The view of the upper part of the right pleural cavity. Huge nodules and neoplastic lymphangitis are visible on the parietal pleura (⚪). Nodules are also present on the surface of the lung (star)
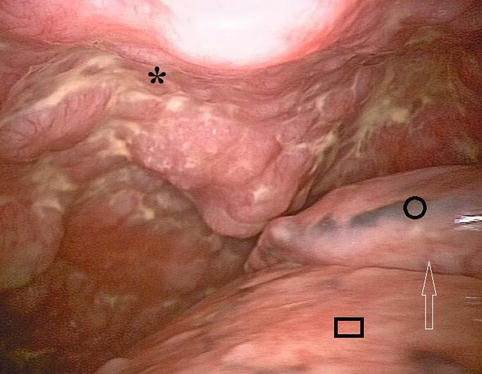
Fig. 10.5
Metastatic pleural cancer (same patient). Posterior parietal pleura (star). Upper lobe (⚪). Lower lobe (◻). Fissure (white arrow)
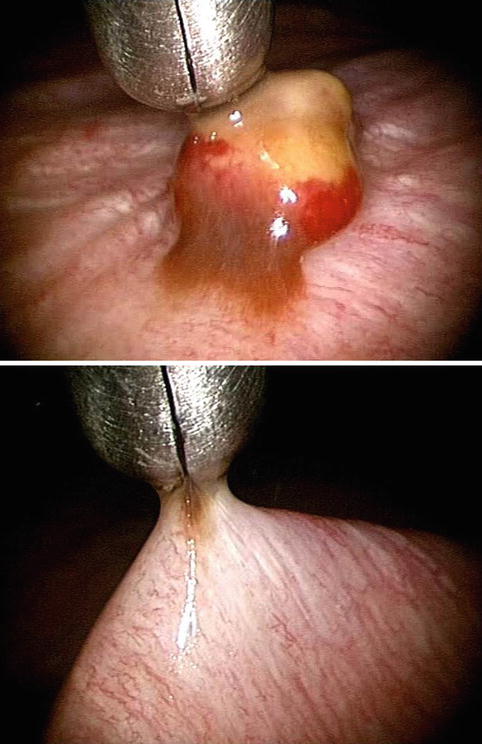
Fig. 10.6
After aspiration of the fluid, a single nodule can be seen. In this case, using an optical biopsy forceps, the nodule located on the diaphragm is removed (adenocarcinoma from primary lung cancer). To perform the procedure with absolute safety, the tip (5 mm) of the forceps has to be visible at all times without any blind periods
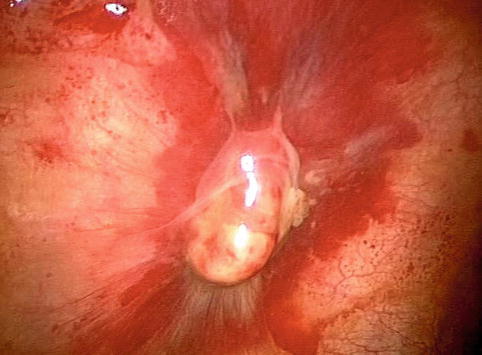
Fig. 10.7
A malignant nodule on the parietal pleura
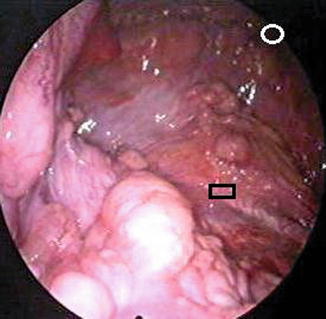
Fig. 10.8
Metastatic pleural adenocarcinoma. No primary cancer was found. Huge nodules are located on the diaphragm. In this case the nodules are not accessible to percutaneous pleural biopsies. (⚪), posterior parietal pleura. (◻), diaphragm

Fig. 10.9
Malignant nodules on the diaphragm. The costal pleura was not invaded by the disease. Previous percutaneous procedures failed to obtain a diagnosis