CT-guided Needle Biopsy
Presentation
A 74-year-old woman is referred to you by her primary medical doctor. She had been living independently up until recently but now requires supervision for progressive somnolence and intermittent confusion. Past medical history is significant for hypertension. She quit smoking 10 years ago after a 50-pack-per-year smoking history. On physical examination, there are no neck masses, the lungs are clear, the heart is regular, and there are no focal neurologic deficits.

Differential Diagnosis
The presenting symptoms of change in mental status could be due to a variety of etiologies, including primary brain lesions, metabolic disturbances, medications, hypoxia, and infection. In this patient with neurologic symptoms and a lung nodule, brain metastases or hypercalcemia as part of a paraneoplastic syndrome should be considered.
Computed tomography (CT) scans of the chest should be obtained to delineate the chest mass. In addition, serum chemistries and a CT scan of the head are required.
Serum Chemistry Results
Serum calcium is elevated at 11.5. CT scan of the head shows no mass lesions.
▪ CT Scans
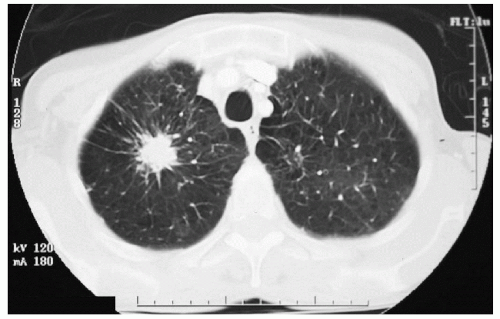 Figure 8-3 |
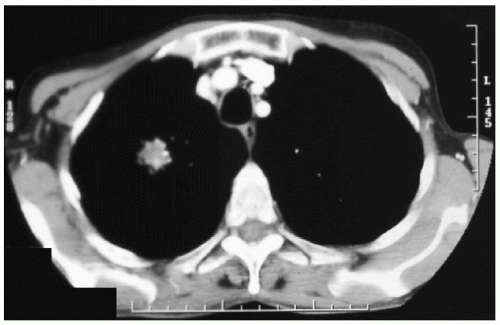 Figure 8-4 |
CT Scan Report
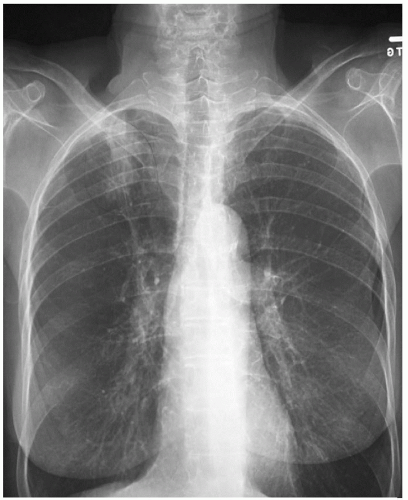
CT scans of the chest demonstrate a 3-cm spiculated mass in the right upper lobe. There are no enlarged mediastinal lymph nodes or pleural effusions.
Discussion
Lung cancer is the leading cause of cancer death in the United States. Although the incidence of lung cancer in men has stabilized, the rates continue to escalate in women, with overall 5-year survival rates of only 10% to 15%.
Tobacco use has been identified as a major risk factor for development of lung cancer by activating oncogenes. Other risk factors include female gender, a diet low in β-carotene, bullous disease, airway obstruction, previous lung cancer, and environmental factors such as secondhand smoke and occupational carcinogens.
In large studies, screening chest x-rays did not improve survival and are not recommended in asymptomatic patients. Presenting symptoms of patients with lung cancer are variable depending on location of the primary lesion and presence of metastatic disease. Most patients are asymptomatic in the early stages. Generally, the disease is advanced if significant symptoms are present. The initial symptoms are usually cough, hemoptysis, wheezing, stridor, dyspnea, or recurrent infections. Extrapulmonary signs and symptoms such as hoarseness, chest pain, dysphagia, pleural effusion, Horner’s syndrome, Pancoast’s syndrome, and superior vena cava syndrome are present in more advanced disease.
Paraneoplastic syndromes can be the first sign of disease. Hypercalcemia, the syndrome of inappropriate antidiuretic hormone (SIADH), and Cushing’s syndrome are the most common. In addition, gynecomastia, galactorrhea, excess growth hormone, increased calcitonin, increased thyroid-stimulating hormone, and hyperglycemia or hypoglycemia can be a manifestation of lung cancer. Squamous cell lung cancer can be associated with hypercalcemia either from bone metastases or para thy roid hormone (PTH)-related protein secretion, although Cushing’s syndrome, SIADH, and gynecomastia can also be associated with squamous cell lung cancer.



