The modern vascular laboratory began in the 1960s with relatively simple physiologic tests performed with inexpensive equipment by vascular surgeons and their staff, usually in an office or clinic setting. Over the last 50 years, the field has expanded in scope to play a key role in the management of patients with vascular problems. As the clinical applications of vascular testing became more numerous and the complexity of the instrumentation increased, the vascular laboratory took on a unique professional identity. Individuals who performed vascular tests became known as “vascular technologists,” and the Society of Non-Invasive Vascular Technology (SNIVT) was established in 1977 to develop and promote this field. In the 1980s, ultrasound imaging became the primary diagnostic method used in the vascular laboratory. Since ultrasound was also being used for a variety of nonvascular diagnostic applications, radiologists, cardiologists, neurologists, and other medical specialists started to take an interest in the vascular laboratory. In 1988, SNIVT changed its name to the Society of Vascular Technology (SVT), and it became the Society for Vascular Ultrasound (SVU) in 2002. The terms “vascular technologist” and “vascular sonographer” are now often used interchangeably.
One consequence of this tremendous growth was the recognition that a specific body of knowledge, training, and experience was required to perform and interpret vascular tests. There was also concern among those in the field that the lack of standards and accountability was resulting in poor-quality and inappropriate vascular testing. Therefore, it was inevitable that some type of regulation would be necessary. Credentialing of personnel and accreditation of vascular laboratory facilities are the two major regulatory processes for addressing these issues.
DEFINITIONS
Credentialing is a general term that describes a formal program for verifying professional knowledge, qualifications, and competence. The credentialing process for individuals includes both certification and licensure. Certification involves the application of private standards, while licensure is based on governmental or public standards. In some situations, the practical difference between certification and licensure may be small, particularly when licensure is based on certification status or passing a privately administered examination. In the United States, licensure is granted at the state level, and in those states with licensing statutes a license is mandatory for an individual to engage in the specified profession. Certification is common among healthcare professions and is well accepted for physicians, nurses, pharmacists, and many other allied health fields. Most certification organizations maintain a registry of individuals who have successfully completed their certification process in order to provide the public with information on appropriately qualified individuals. Licensure also applies to many healthcare professions, although licensure for sonographers is a relatively recent development. Several states now have sonography licensure, and many others are considering such requirements. Both certification and licensure are typically time-limited designations with specific requirements for maintaining credentialed status, such as continuing education or retesting. Accreditation can be considered as a form of credentialing, but it is applied to programs or facilities, rather than individuals.
The organizations offering credentialing and accreditation for the vascular laboratory are listed in Table 3.1. This chapter discusses the most widely recognized credentialing and accreditation pathways through the American Registry for Diagnostic Medical Sonography (ARDMS) and the Intersocietal Accreditation Commission (IAC) Vascular Testing.
THE AMERICAN REGISTRY FOR DIAGNOSTIC MEDICAL SONOGRAPHY
The ARDMS was incorporated in 1975 as an independent nonprofit organization to provide certification examinations in the various specialties of medical sonography. In addition to vascular technology, these now include abdomen, breast, neurosonology, obstetrics and gynecology, musculoskeletal sonography, and adult, pediatric, and fetal echocardiography (Table 3.2). The ARDMS has also developed a credential for physicians who interpret vascular laboratory tests—Registered Physician in Vascular Interpretation (RPVI). Although physicians can be eligible to take the examinations leading to the ARDMS sonography credentials, the RPVI is the first credential created specifically for physicians. As of late in 2013, the ARDMS has certified over 80,000 individuals, including more than 24,000 vascular technologists and about 2000 interpreting physicians. As a member of the National Commission for Certifying Agencies, the ARDMS examinations are required to be “practice based,” that is, they must reflect current practice in diagnostic ultrasound. To make sure that this requirement is met, periodic “job task analysis” surveys are conducted to document the status of the various ultrasound specialties. These surveys are made available online to ARDMS registrants in a particular specialty and cover all aspects of ultrasound practice relevant to that specialty. The results of these surveys determine the topics covered and the content of the questions for the examination.1,2,3
TABLE 3.1 ORGANIZATIONS OFFERING CREDENTIALING AND ACCREDITATION FOR THE VASCULAR LABORATORY
Credentialing for Personnel
American Registry for Diagnostic Medical Sonography (ARDMS)
Cardiovascular Credentialing International (CCI)
American Registry of Radiologic Technologists (ARRT)
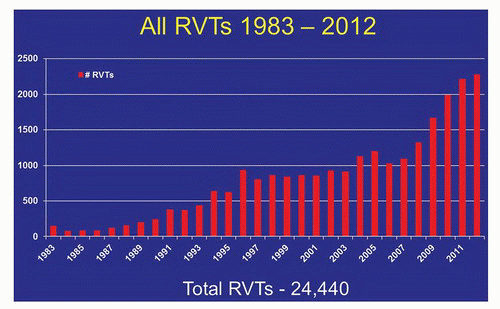
Between 1975 and 1982, the ARDMS offered a certification examination in Peripheral Vascular Doppler. The Registered Vascular Technologist (RVT) examination was first administered in 1983, and through 2012 more than 24,000 individuals have obtained the RVT credential (Fig. 3.1). A survey conducted by the SNIVT in 1982, along with the 1988, 1994, 2000, 2005, and 2009 ARDMS vascular technology task surveys, documents the changes that have occurred in this specialty.
TABLE 3.2 SONOGRAPHY EXAMINATIONS AND CREDENTIALS OFFERED BY THE ARDMS
▪ EXAMINATIONS
▪ CREDENTIALS
▪ PHYSICS
▪ SPECIALTY
SPI
Sonography Principles & Instrumentation
Examination
Abdomen (AB)
RDMS
Registered Diagnostic Medical Sonographer
Breast (BR)
Fetal Echocardiography (FE)
Neurosonology (NE)
Obstetrics and Gynecology (OB/GYN)
Adult Echocardiography (AE)
RDCS
Registered Diagnostic Cardiac Sonographer
Fetal Echocardiography (FE)
Pediatric Echocardiography (PE)
Vascular Technology (VT)
RVT
Registered Vascular Technologist
MSK
Musculoskeletal Sonography
Examination
RMSK
Registered in Musculoskeletal
PVI
Physicians’ Vascular Interpretation
Examination
RPVI
Registered Physician in Vascular Interpretation
Both the SPI and a specialty examination are required for the RDMS, RDCS, and RVT credentials. The RMSK and RPVI credentials require a single examination that includes some physics content.
The 1982 SNIVT Survey
In 1982, ankle and segmental blood pressures were the most common examination methods for peripheral arterial disease, while continuous-wave Doppler and impedance plethysmography were the most widely used tests for deep vein thrombosis. Testing methods for extracranial carotid artery disease included phonoangiography, periorbital Doppler, and pressure or pulse delay oculoplethysmography. Patients were frequently subjected to multiple tests for a single vascular problem. B-mode or duplex imaging was used by less than 25% of the surveyed technologists and only for the diagnosis of carotid artery disease.1
The 1988 ARDMS Vascular Technology Task Survey
The most striking change in vascular technology between 1982 and 1988 was the growth of duplex scanning as a primary testing method.2 According to the 1988 ARDMS survey, 96% of RVTs used duplex imaging; however, only 24% had access to color-flow instrumentation. The indirect testing methods were still widely used for peripheral arterial and venous disease, although 23% of RVTs were performing duplex scanning of the peripheral arteries and 75% of RVTs reported using duplex scanning for evaluation of lower extremity bypass grafts. Duplex scanning was the predominant technique for extracranial carotid artery testing, with only about one-half of RVTs still performing indirect cerebrovascular testing. Transcranial Doppler was being used by 17% of RVTs.
The 1994 ARDMS Vascular Technology Task Survey
The 1994 ARDMS survey indicated that 93% of RVTs utilized some form of duplex scanning with color-flow imaging.3 While the use of indirect peripheral arterial tests declined slightly, arterial duplex scanning was used by 86% of RVTs. For venous testing, 95% of RVTs used duplex imaging for diagnosis of deep vein thrombosis, and 82% performed duplex saphenous vein mapping. Continuous-wave Doppler was still used by 69% of RVTs, but only about 10% reported using plethysmographic methods for venous disease. The indirect cerebrovascular tests continued to decline, with about 14% of RVTs using oculoplethysmography and 30% performing the periorbital Doppler test. Duplex scanning with color-flow imaging was used by 98% of RVTs for carotid evaluation. The use of transcranial Doppler among RVTs increased only slightly to 20%.
FIGURE 3.1. Annual numbers of individuals obtaining the RVT credential from 1983 through 2012.
The 2000 ARDMS Vascular Technology Task Survey
In the fall of 1999, the ARDMS conducted its first “online” task survey for vascular technology. Among the responding RVTs, 41% were working in accredited vascular laboratories. It is noteworthy that approximately 90% of RVTs provided preliminary interpretations of examinations to referring physicians. Duplex imaging with color flow was used by 98% of RVTs for one or more applications. About 70% of RVTs measured segmental pressure gradients in the lower extremities, and 88% used duplex imaging to assess the lower extremity arteries. Mesenteric and renal artery duplex scanning were performed by 51% and 63% of RVTs, respectively. About 4% of RVTs reported using impedance plethysmography for lower extremity venous evaluation. For the extracranial carotid evaluation, less than 10% of RVTs still performed periorbital Doppler testing, while only about 2% used any type of oculoplethysmography. Duplex scanning with color-flow imaging was used by 98% of RVTs for carotid testing. The use of transcranial Doppler among RVTs remained around 20%. About 25% of RVTs performed some type of intraoperative monitoring by duplex scanning.
Only gold members can continue reading. Log In or Register to continue