(1)
Department of General surgery, Fuwai Hospital, Beijing, China
26.1 General Considerations
26.1.1 Definition
Corrected transposition of the great arteries (CTGA) is a condition in which the connections of the great artery valves with the ventricles are inverted, as are the atrium-ventricle connections (Fig. 26.1a, b). Oxygenated blood of the morphological LA can still flow into the morphological RV and be pumped into the aorta; therefore, the blood flow is functionally corrected and clinical cyanosis will not occur.
26.1.2 Classification
Classification of complete TGA and CTGA (connection of great arteries and ventricles are completely inverted, excluding double outlet of the ventricle) are as below:
Usual classifications of complete anomalous arterial ventricular connection (not including partial anomalous connection)
Complete transposition of the great arteries with normal atrioventricular connection | Functionally corrected transposition of the great arteries with atrioventricular discordance | |||||||
|---|---|---|---|---|---|---|---|---|
Situs | Solitus | Inversus | Solitus | Inversus | ||||
Ventricle | Dextro- | Levo- | Levo- | Dextro- | ||||
Transposition of the great arteries | RA | LA | LA | RA | RA | LA | LA | RA |
RV | LV | LV | RV | LV | RV | RV | LV | |
P | P | P | P | |||||
A | A | A | A | |||||
TGA | TGA | CTGA | CTGA | |||||
CTGA, because it has been functionally corrected and the aorta still receives pulmonary vein blood and the pulmonary artery still receives blood from the systemic veins, is clinically asymptomatic only until tricuspid insufficiency occurs. The insufficiency occurs when the patient has grown into childhood or adulthood, and the TV no longer is able to withstand the long-term load of the systemic circulation. If it coexists with another intracardiac abnormality and requires surgery, the anatomical characteristics should be given thorough consideration.
26.2 Surgical Considerations
26.2.1 Cardiac Appearance and Course of the Coronary Artery
The left and right atria are situs, but the left and right ventricles are bilaterally side by side, and the ventricular septum is nearly sagittal (Fig. 26.1a). Thus, the anterior interventricular groove is closer to the median line than in the normal heart. The ascending aorta lies to the left anteriorly, and the pulmonary artery lies to the right and posteriorly. The coronary arteries originate from the left and right aortic sinus, and the noncoronary sinus (posterior sinus) is moved to the anterior. The anterior descending branch originates from the main trunk of the RCA.
26.2.2 Atrioventricular Ring and the Membranous Septum
The atrium of the (situs solitus,L-loop, L- transposition) SLL type of CTGA is situs, but the ventricular chamber of the right side is a MV ventricle (Fig. 26.1c), with the adherent fringe of the MV at the ventricular septum still higher than the contralateral adherent fringe of the tricuspid septal leaflet. The membranous septum lies inferior to the MV ring. Therefore, in a dissected cardiac chamber, the membranous septum can be seen to lie inferior to the right atrioventricular ring (MV ring), which is contrary to the right ventricle view in the normal heart.
26.2.3 Complete Muscular Cone Inferior to the Aortic Valve
The AV and the left TV ring are separated by muscular tissue. Contrariwise, the PV is connected by fibrous tissue with the MV to the right. A supraventricular crista-like bundle can be seen from the left side of ventricular septum (Fig. 26.1d).
26.2.4 Anatomical Connection of the Pulmonary Artery Outflow
The pulmonary artery outflow of the CTGA is an oblique canal that lies deeply between the inverted MV and TV ring (Fig. 26.1e). The PV ring is conjuncted [connected?] with the posterior central fibrous body. It is fibrously connected with the MV ring to the right, and its left side is the membranous septum (Fig. 26.1f). It lies anteriorly next to the AV ring with the conical ventricular septum. The PV ring rides just over the muscular ventricular septum.
26.2.5 Course of the Conducting System
The conducting system of a CTGA originates from the anterior atrioventricular node, which is located at the junction point of the pulmonary and mitral valves and also where the atrial septum connects with the right auricle (Fig. 26.1g). The conducting bundle travels from the anterior border of the PV ring to the superior border of the muscular ventricular septum; it then divides into the left and right bundles. The left bundle is located in the anatomical LV, whereas the right bundle travels downward into the anatomical RV. If there is a membranous VSD, the right bundle will travel at the anterior border of the defect, whereas in the normal heart, the conduction system travels along the posterior and inferior border of the defect. When suturing a VSD in CTGA, the anterior and superior border of the defect is a dangerous zone where the conducting bundle is easily injured and can cause atrioventricular block.
26.3 Specimen Demonstration
26.3.1 CTGA + VSD, Typical Type
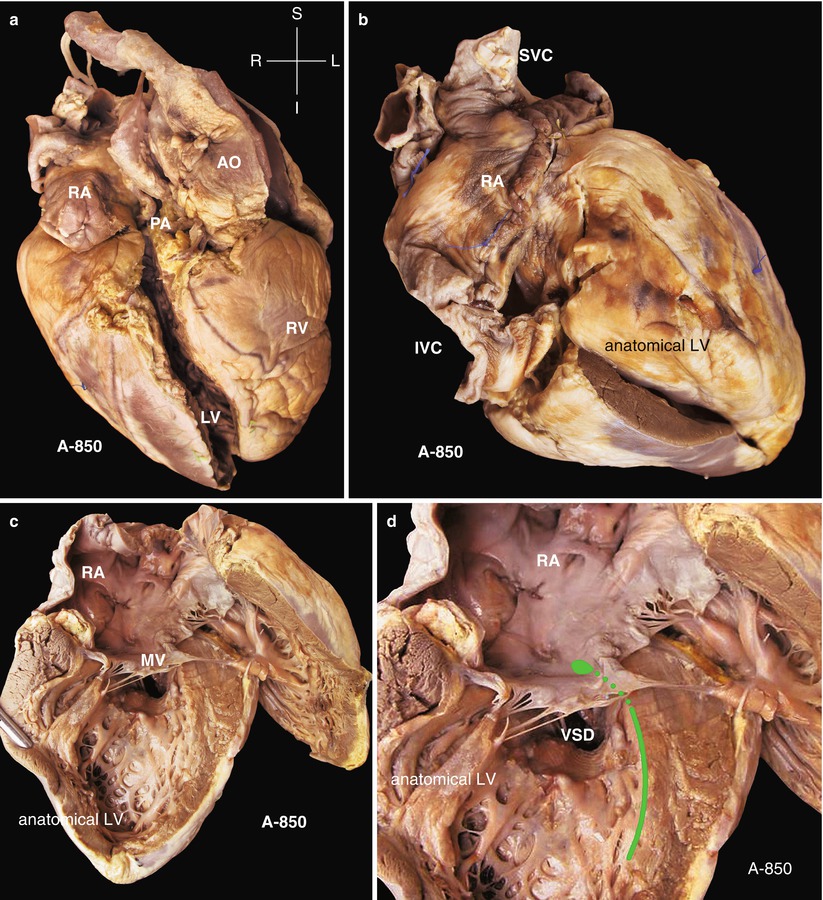
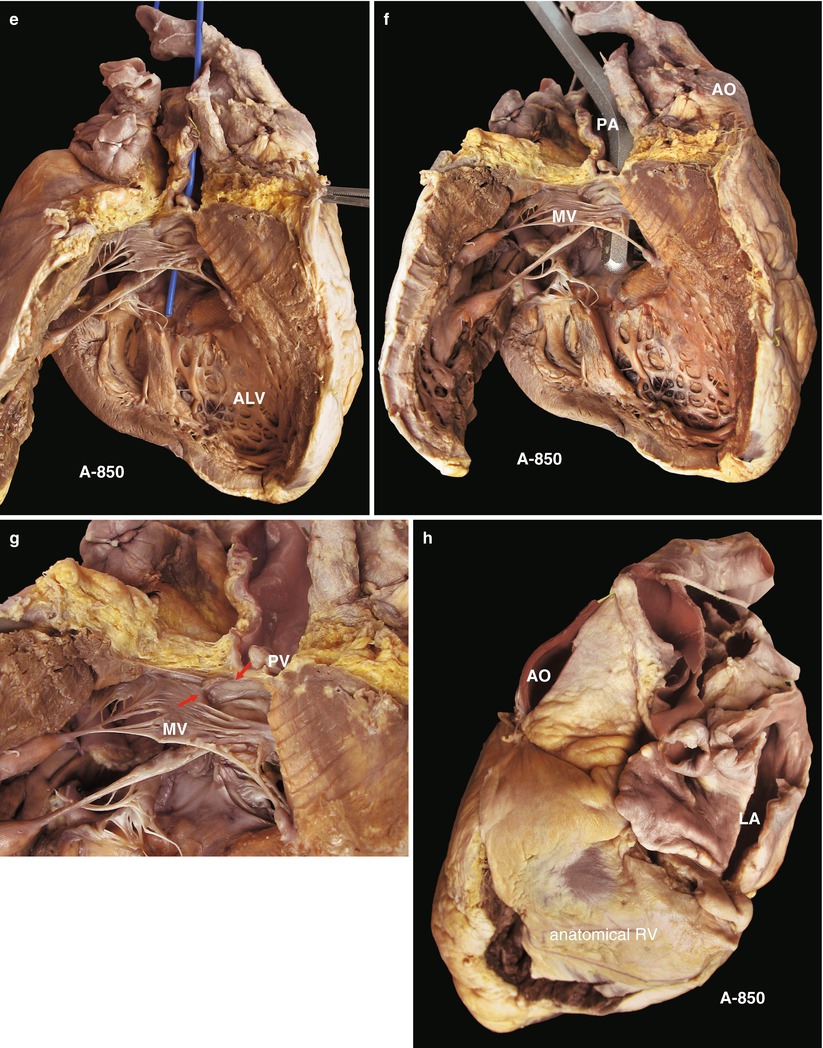
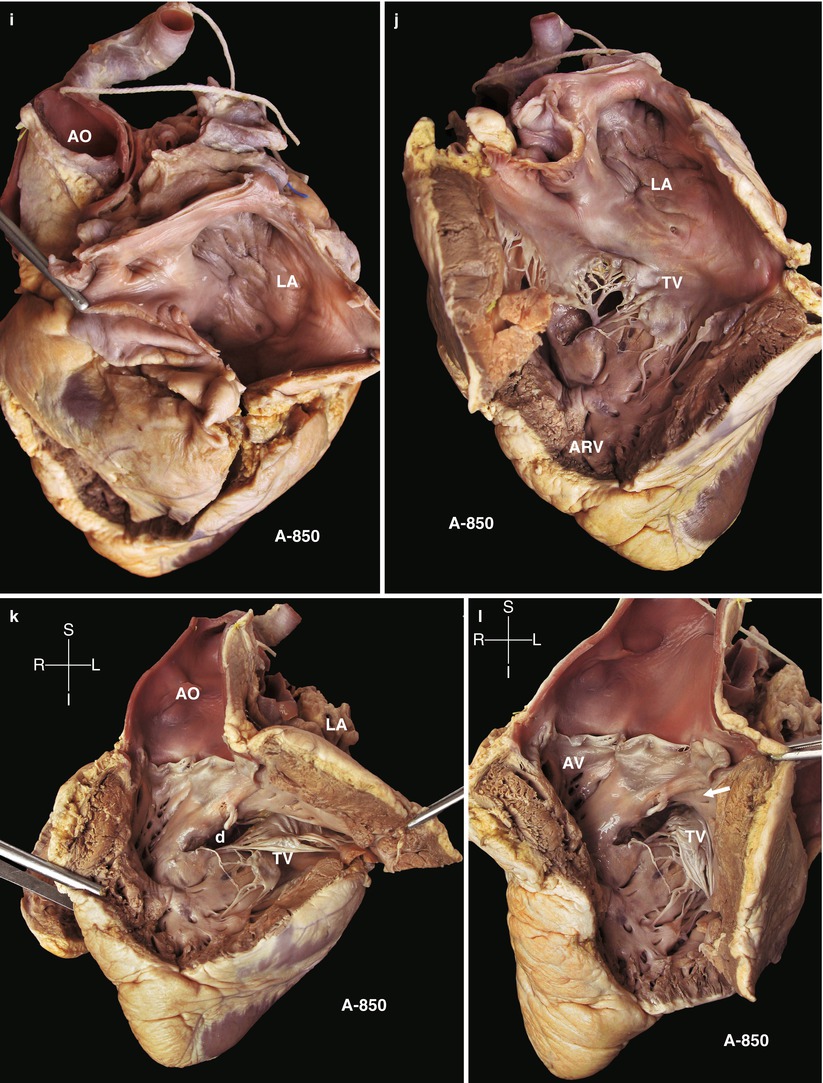
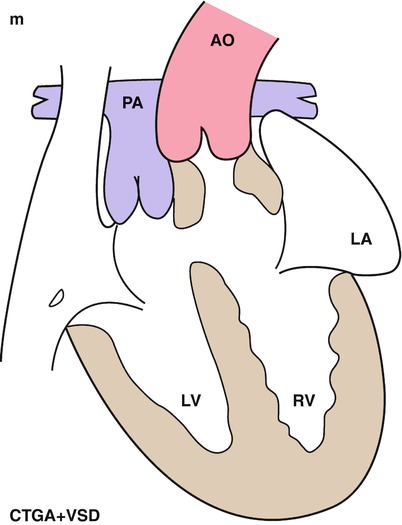
Fig. 26.1
(a) Specimen 850. Anterior view of CTGA. The pulmonary artery is located right and posterior to the aorta, whereas the RA remains at the right side, which belongs to the situs solitus. AO ascending aorta; LV left ventricle; PA main pulmonary artery; RA right atrium; RV right ventricle. (b) Specimen 850. The RA is connected with the morphological LV or anatomical LV. IVC inferior vena cava; RA right atrium; SVC superior vena cava. (c) Specimen 850. Atrium and ventricle of the right side are dissected. The superior is the RA, and the atrioventricular valve is the MV. The inferior is a morphological LV (or an anatomical LV). (d) Specimen 850. Ventricular septal defect and the anterior border of the defect. The conducting bundle travels underneath the endocardium from the anterior atrioventricular node (green line) and along the anterior and superior border of the VSD. RA right atrium. (e) Specimen 850. The outflow of the morphological LV (ALV) extends directly into the pulmonary artery (blue probe). (f) Specimen 850. A thick probe is inserted into the morphological LV from the pulmonary artery. A VSD can be detected at the same time. MV mitral valve, PA pulmonary artery, AO ascending aorta. (g) Specimen 850. Figure demonstrates the fibrous connection of mitral and pulmonary valves (arrow). MV mitral valve, PV pulmonary valve. (h) Specimen 850. Observing the LA and left-side ventricle. The left-side ventricle is the morphological RV, which connects with the AV. AO ascending aorta, LA left atrium. (i) Specimen 850. Showing the left-side atrium and ventricle. The atrium (LA) has been dissected, showing the unsmooth surface of the atrium septum. The LA is connected with the morphological RV. (j) Specimen 850. The ventricular wall has been lifted, and the ventricular inflow can be seen. The TV has been completely unfolded, and a VSD can be seen subvalvularly. The ARV is the morphological RV. LA left atrium. (k) Specimen 850. Figure demonstrates that the aorta (AO) originates directly from the left ventricular outflow. There is a muscular septum between the aorta and TV, the structure of which equals the supraventricular crista, beneath which is the VSD (d). LA left atrium, AO ascending aorta, D ventricular septal defect, TV tricuspid valve. (l) Specimen 850. Figure demonstrates the connection between the AV and the TV. The TV has three leaflets with many small pores at the border of the leaflets, which is a variance of the leaflet development. Because the pores lie above the closing line, they seldom cause insufficiency. The aortic and the tricuspid valves are separated by the supraventricular crista, beneath which is the VSD, with its border adhered by chordae tendineae (arrow). (m) Schematic diagram of specimen 850. Atria are solitus, whereas the ventricles and atrioventricular valves are inversus. The aorta originates from the morphological RV, and the pulmonary artery originates from the morphological LV, with a muscular-type VSD. PA pulmonary artery, AO ascending aorta, LA left atrium
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


