Coronary Artery Disease and Regional Left Ventricular Function
Chapter 15 looked at the global assessment of left ventricular (LV) dimensions and function. However, abnormalities of LV function can affect one or more specific areas of the LV wall and then the LV is said to show a regional wall motion abnormality (RWMA). RWMA is the result of coronary artery disease affecting the function of the myocardium, either because the blood supply to a particular area of myocardium has become reduced (ischaemia) or blocked altogether, causing death (necrosis) of the myocytes. The identification of RWMA by echo can therefore reveal a great deal about the status of the coronary circulation.
THE CORONARY ARTERIES
Normal coronary artery anatomy
As discussed in Chapter 2, the coronary circulation normally arises as two separate vessels from the sinuses of Valsalva – the left coronary artery (LCA) from the left sinus, and the right coronary artery (RCA) from the right sinus (Fig. 2.5, p. 9). The initial portion of the LCA is the left main stem which soon divides into the left anterior descending (LAD) and circumflex (Cx) arteries. The LAD runs down the anterior interventricular groove and the Cx runs in the left atrioventricular groove. The RCA runs in the right atrioventricular groove, and in most people gives rise to the posterior descending artery which runs down the posterior interventricular groove.
All the arteries supply branches to the myocardium in their respective territories, and as there is some anatomical variation from one person to the next, there can be a little variability in which vessel is responsible for supplying blood to each territory. Nonetheless, each vessel’s territory is fairly well defined and so wall motion abnormalities in a particular region give an indication of the coronary vessel(s) likely to be involved.
Regional left ventricular function
The LV is conventionally split into 16 or 17 different regions or ‘segments’. In the 16-segment model the LV is sliced longitudinally into thirds (basal, mid-cavity and apical). The basal and mid-cavity slices each contain six segments and the apical slice contains four segments. The American Heart Association’s 17-segment model contains all these segments plus one more – an apical ‘cap’ (Fig. 16.1). The 16-segment model remains popular for echo purposes, but if you are going to compare echo findings with other modalities (e.g. nuclear cardiology) then it is better to use the more widely applicable 17-segment model. Whichever model you choose, ensure that your nomenclature is consistent.
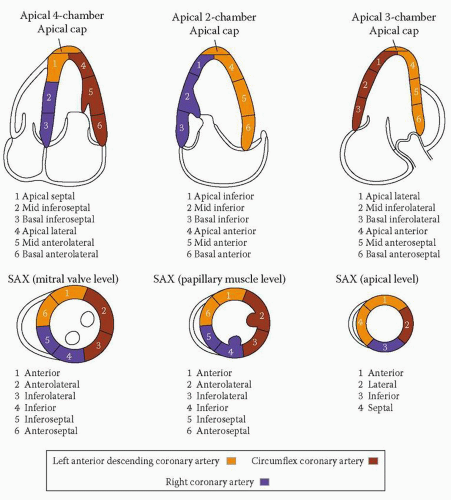 Figure 16.1 The 17-segment model of LV segmentation (SAX = short axis) |
In the 17-segment model, the six segments in each of the basal and mid-cavity slices are termed anterior, anteroseptal, inferoseptal, inferior, inferolateral (sometimes also called posterior) and anterolateral. The boundaries of the septum are defined by the attachment of the right ventricle (RV), and each of the six circumferential segments occupies 60° in the short axis view. As the LV narrows towards the apex, there are just four apical segments, termed anterior, septal, inferior and lateral. The apical cap is at the very tip of the ventricle, where there is no LV cavity.
Each segment is assigned to one of the coronary arteries (LAD, Cx or RCA), as indicated by the colour-coding in Fig. 16.1, although there can be some overlap depending on each individual’s coronary anatomy. Normal wall motion during systole is indicated by an endocardial excursion >5 mm and by wall thickening >50 per cent. Inspect each segment in turn, where possible in two separate views, and score it according to its motion:
MYOCARDIAL ISCHAEMIA AND INFARCTION
Myocardial ischaemia results from the development of an atherosclerotic plaque in one or more coronary arteries, limiting the flow of blood to the myocardium downstream. This normally does not cause symptoms until the lumen is obstructed by ≥70 per cent, at which point the patient develops exertional chest discomfort and/or breathlessness. The chest discomfort is typically central in location and heavy or tight in character, and may radiate into the neck and jaw and down one or both arms. The symptoms are rapidly relieved with rest and/or nitrates.
An acute coronary syndrome occurs when an atherosclerotic plaque ruptures, exposing the lipid-rich core to the bloodstream. This leads to the rapid formation of a thrombus which acutely obstructs flow down the coronary artery. If this leads to necrosis of a portion of myocardium, cardiac markers (e.g. troponins) will be released into the circulation, and the detection of these markers is one of the key diagnostic features of a myocardial infarction. Unstable symptoms without a rise in cardiac markers is termed unstable angina.
Echo assessment of myocardial ischaemia and infarction
Areas of myocardial ischaemia and infarction typically lead to hypokinetic, akinetic, dyskinetic or aneurysmal myocardial segments. By assessing wall motion in each of the LV segments a comprehensive picture of LV




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
