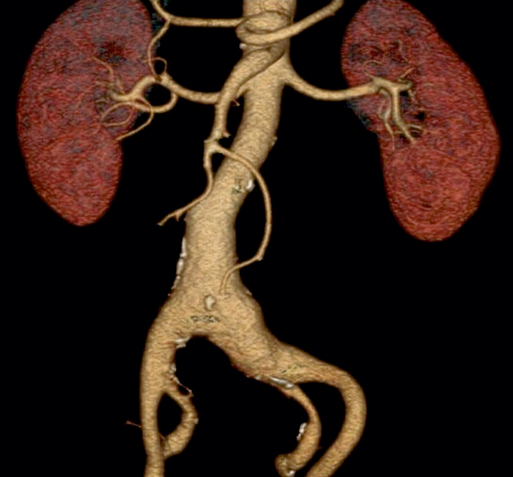
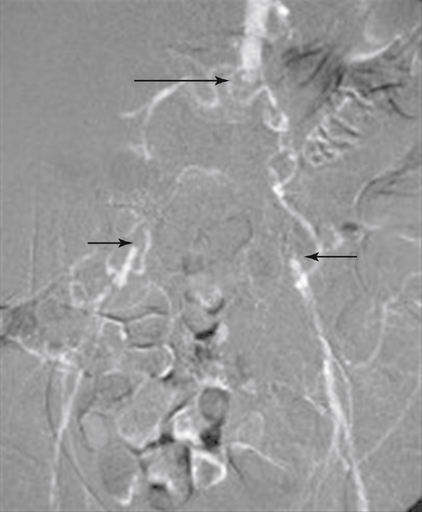
Patients with borderline kidney function no longer pose as much of a challenge to conventional angiography because carbon dioxide DSA and catheter manometry provide the necessary image and physiologic data to guide therapy (Figure 1). Carbon dioxide can be safely used for all aortoiliac imaging and therapy, as well as for completion images when iodinated contrast use must be minimized. Carbon dioxide use is contraindicated for imaging the central nervous system. CTA was developed in the early 1990s following the introduction of spiral (or helical) CT scanning. CTA for vascular diagnosis has become the favored imaging modality for evaluating aortoiliac occlusive disease (Figures 2 to 6).
Conventional Arteriography, Magnetic Resonance Angiography, and Computed Tomographic Arteriography of Aortoiliac Occlusive Disease
Digital Subtraction Arteriography
Computed Tomography Angiography
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine