CT has emerged as a very important imaging modality for penetrating neck trauma. Its utility lies in part in the evaluation of aerodigestive tract injury, although these injuries have a higher false-positive rate than vascular injuries, in which the sensitivity and specificity for arterial injuries are both greater than 95%. Metal artifacts from ballistic injury limit the utility of CT in some patients. CT has been demonstrated to accompany decreased rates of unnecessary neck exploration and limits the need for oesophagogram or catheter-based arteriogram. If CT demonstrates ballistic trajectories that are remote from important structures then additional invasive imaging can be avoided. CTA is also a useful for preoperative planning when the patient’s stability permits and there is need for clarification of the best surgical approach (Figures 1 and 2). CTA has clearly emerged as the screening modality of choice with blunt injury to the aorta. In contrast, the benefit of CTA is less clear with penetrating vascular injuries to the chest. The majority of penetrating injuries to the chest occur from knife wounds or projectiles from handguns. Injuries from nail guns and other atypical injuries have also been reported. Penetrating wounds that traverse the mediastinum are often lethal as a result of involvement of the heart and great vessels, whereas those that are outside the mediastinum typically do not result in vascular injury, but rather cause pulmonary, chest wall, and diaphragm wounds. Nevertheless, CTA is useful in patients in whom the missile trajectory crosses the midline and can involve the mediastinum. If these patients are hemodynamically stable, CTA can aid with determining patients in whom expeditious operation is warranted, patients who warrant aerodigestive tract evaluation, and those patients in whom diagnostic angiography may be of benefit (Figure 3).
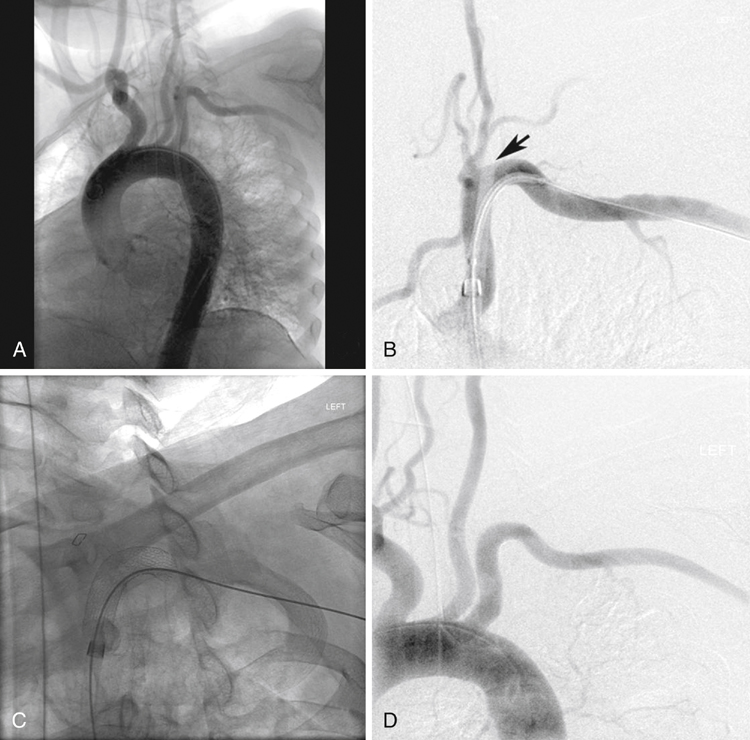
Conventional and Computed Tomographic Arteriography in Penetrating Vascular Injuries
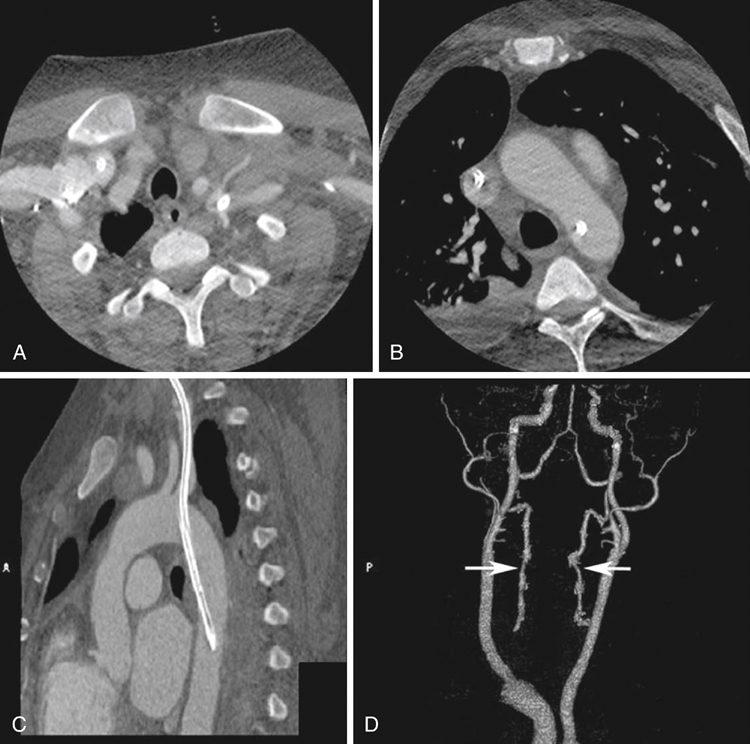
Imaging for Penetrating Vascular Injuries of the Neck
Imaging for Penetrating Vascular Injuries of the Thorax
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine

