Chapter 30 Congenital Pulmonary Arteriovenous Fistula
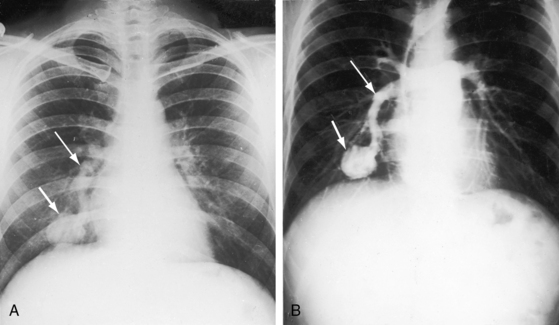
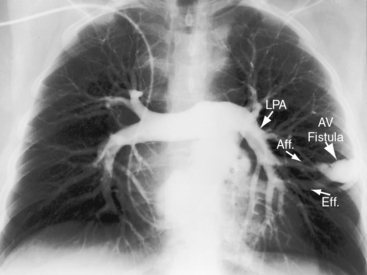
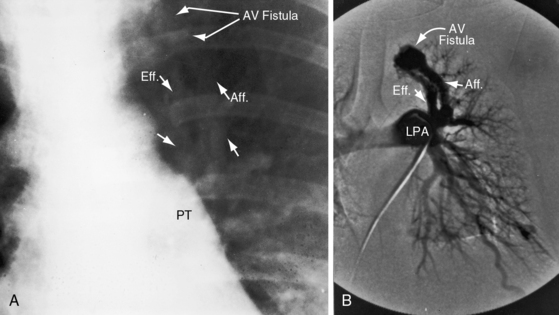
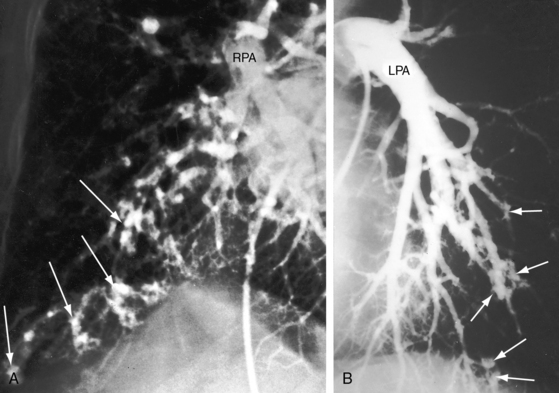
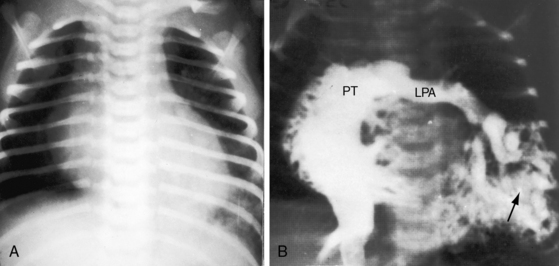
In 1897, the British Medical Journal published a necropsy description of congenital pulmonary arteriovenous fistulae,1 and four decades later, the anomaly was recognized in a living subject.2 Pulmonary arteriovenous fistulae are the result of an embryonic fault in the vascular complex that is responsible for the development of pulmonary arteries and veins.3 The fistulae can be solitary or multiple, unilateral or bilateral, or minute and diffuse throughout both lungs.4–6 Approximately 75% of congenital pulmonary arteriovenous fistulae involve the lower lobes or right middle lobe (Figures 30-1 through 30-5)4,7; they usually occur without coexisting congenital heart disease. Isolated exceptions have been reported with left isomerism (see Chapter 3)8,9 and with atrial septal defect (see Chapter 15).10 Estimated minimal prevalence rate is 1/10,000 births.11


In 1865, Babington12 called attention to familial epistaxis; and in 1876, Legg13 described recurrent epistaxes and cutaneous telangiectasia in three generations. Twenty years later, Rendu14 published his classic description of familial epistaxes and telangiectasia (cutaneous angiomatas) of the nose, cheeks, and upper lip. In 1901, Osler15 reported on a “family form of recurring epistaxis associated with multiple telangiectases of the skin and mucous membranes”; and in 1907, Weber16 reported “multiple hereditary developmental angiomata (telangiectases) of the skin and mucous membranes associated with recurring haemorrhages.” In 1909, Hanes17 referred to the disorder as hereditary hemorrhagic telangiectasia,18 but the eponym Rendu, Osler, Weber remains in use without the inclusion of Legg13 and with no consensus about the most appropriate sequence of names.19,20 The diagnosis of hereditary hemorrhagic telangiectasia (HHT) is made clinically with the Curaçao criteria, which was established in 1999 by the Scientific Advisory Board of the HHT Foundation International. The criteria include recurrent epistaxis; telangiectases of the lips, oral cavity, fingers, and nose; gastrointestinal telangiectasia; and pulmonary, hepatic, cerebral or spinal arteriovenous malformations.19,21,22
A fistula consists of either one or more relatively large vascular trunks, a thin aneurysmal sac, or a tangle of distended tortuous vascular channels (Figures 30-1 through 30-7).18 The arterial supply is through enlarged tortuous branches of a pulmonary artery, and drainage is through dilated pulmonary veins (see Figures 30-1 through 30-4 and 30-6).3,23 Fistulous rupture results in hemorrhage into the pulmonary parenchyma or into the pleural space.24 Exceptionally, the arterial supply is from a bronchial, intercostal, anomalous systemic artery or a coronary artery (see Chapter 22). The fistula is then systemic arteriovenous rather than pulmonary arteriovenous.18 A rare anatomic variation consists of a congenital connection between a pulmonary artery and the left atrium, an anomaly in which an initial connection exists between a pulmonary artery and a pulmonary vein; but during vascular development, the pulmonary vein becomes incorporated into the left atrium.25–29 Extralobar arteriovenous fistulae are represented by pulmonary sequestrations in which the arterial supply and venous drainage are systemic rather than pulmonary. Isolated congenital varicose pulmonary veins are rare and not the result of arteriovenous malformations.30
The physiologic consequences of pulmonary arteriovenous fistulae depend on the amount of unoxygenated blood delivered through the malformation and on the size of the malformation, which tends to increase with age.31,32 Although the volume of blood delivered through the fistula is sufficient to cause cyanosis, it is rarely sufficient to impose a physiologic burden (see Figure 30-7). Pulmonary artery pressure is normal, with rare exception.33 In experimental pulmonary arteriovenous fistulae, cardiac output and left ventricular stroke volume are increased,34 but in congenital pulmonary arteriovenous fistulae, blood flow through the malformation is increased while flow through uninvolved lung decreases by a comparable amount. Accordingly, the net volume of blood that reaches the left side of the heart is little if at all affected, so left ventricular stroke volume and cardiac output remain normal or nearly so. Rarely, a large pulmonary arteriovenous malformation imposes an excess volume load on the left side of the heart and induces congestive heart failure (see Figure 30-7).
Blood flow through pulmonary arteriovenous fistulae is affected by mechanical factors.35 Flow through lower lobe fistulae is augmented in the upright position because of increased perfusion of dependent portions of the lungs. A decubitus position compresses the dependent lung and reduces blood flow through an ipsilateral fistula. A case in point was a large pulmonary arteriovenous fistula in an infant in whom ipsilateral chest wall compression was therapeutic, immediately decreasing the cyanosis and relieving the dyspnea (see Figure 30-7). Elevation of the diaphragm during pregnancy can compress a lower lobe fistula and abolish the accompanying murmur, which reappears after delivery.35
Acquired pulmonary arteriovenous fistulae are occasional sequelae of cavo-pulmonary shunts, especially Glenn shunts.36,37 Acquired fistulae occur in children with hepatic cirrhosis and portal hypertension, especially with biliary atresia and right isomerism (see Chapter 3),38,39 and regress after liver transplantation.38 Large hepatic arteriovenous fistulae sometimes occur without pulmonary arteriovenous fistulae in Rendu-Osler-Weber disease.40–42 Hepatic, cerebral, and pulmonary arteriovenous fistulae may coexist.43
In 1917, telangiectasia and epistaxes were reported in a patient who died of massive hemothorax and at necropsy had three pulmonary arteriovenous fistulae.44 The association of hemorrhagic telangiectasias with pulmonary arteriovenous fistulae has been amply confirmed.4,5,18,19 Hereditary hemorrhagic telangiectasis is an autosomal dominant vasculopathy.11 Clinical diagnostic criteria have changed remarkably little in the last century.19
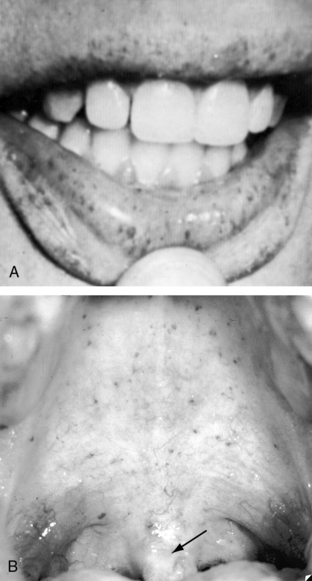
Pulmonary arteriovenous fistulae occur in 5% to 30% of patients with telangiectasia, and telangiectasia occur in 30% to 60% of patients with pulmonary arteriovenous fistulae.45 The incidence rate of pulmonary arteriovenous fistulae with telangiectasia is 1:50,000 with autosomal dominant transmission and a 20% mutation rate. The mucocutaneous lesions are tiny localized arteriovenous fistulae composed of thin dilated vascular membranes with a layer of endothelium and no muscular or elastic coat.18,46 The lesions are fragile and rupture easily.18 Telangiectasia are found on the skin, the lips (Figure 30-8), and the nasal, oral and vaginal mucous membranes; beneath the nails; and in the gastrointestinal tract, liver, central nervous system, kidney, and retina.18,47–49
History
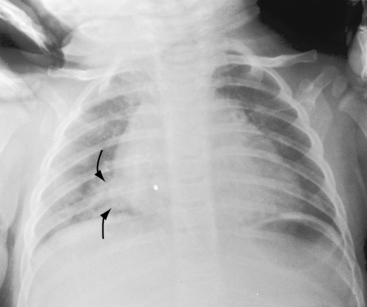
Pulmonary arteriovenous fistulae and hereditary hemorrhagic telangiectasia afflict males and females with equal frequency.18,50,51 The fistulae tend to increase in size and number with the passage of time31,32 and are seldom recognized until adulthood.50,52 Symptoms are the same whether the malformations are multiple or single (see Figures 30-1, 30-2, and 30-3), except for minute diffuse fistulous channels (see Figures 30-4 and 30-5). Mean patient age in a large series was 39 years (range, 3 years to 73 years), with a distinct majority over age 20 years. However, the first description of a pulmonary arteriovenous fistula was at necropsy in a 12-year-old boy (see previous).1 Despite adult prevalence, cyanosis is occasionally present shortly after birth,53 and the malformation is occasionally overtly manifest in childhood (Figure 30-9).53
Asymptomatic acyanotic pulmonary arteriovenous fistulae usually come to light because of abnormal shadows on a routine chest x-ray. Symptoms and complications are related to the pulmonary malformation per se or to coexisting hereditary hemorrhagic telangiectasia.34,54 Congestive heart failure is reserved for infants with a rare large fistula (see Figure 30-7). The right-to-left shunt inherent in the fistulous communication results in cyanosis but seldom causes significant symptoms.53 Dyspnea and fatigue are the result of anemia provoked by bleeding telangiectasia. Rupture of fistulae into a contiguous bronchus causes hemoptysis that varies from mild and occasional to recurrent and massive.55,56 Fistulae are rarely substrates for infective endocarditis.23 Chest pain accompanies pleural involvement. Hemothorax results from rupture of a subpleural fistula.18,23,24,55,57 Intrapulmonary hemorrhage can be massive and fatal.58 Pregnancy is accompanied by adverse effects that resolve after delivery, including hemothorax,59 hemoptysis,60,61 enlargement of existing fistulae, increasing cyanosis,59,61 and expansion of occult fistulae.62 However, pregnancy exerts favorable effects, such as compression of lower lobe fistulae, because of elevation of the diaphragm.35
Epistaxes are the most frequent and usually the first overt hemorrhagic event.18 Cutaneous lesions bleed easily, especially when exposed to sunlight.18 Tracheobronchial telangiectases set the stage for hemoptysis,18 and appropriately placed lesions elsewhere cause melena, hematuria, intraocular hemorrhage, vaginal bleeding, and cerebrovascular accidents.18,48,46
Gastrointestinal endoscopy detects mucosal telangiectases.22 Cerebral events special deserve comment with reference to a peculiar constellation of symptoms, including dizziness, vertigo, paresthesiae, tinnitus, faintness, visual disturbances, speech defects, headache, weakness of the limbs, hemiplegia, mental confusion, and convulsions.35,18 Cerebral episodes may be brief or prolonged, isolated or recurrent, and tend to manifest similar patterns with subsequent attacks.18 Pathogenesis has not been established, but occurrence in acyanotic patients without pulmonary arteriovenous fistulae incriminates telangiectasias,18 which have been described with a cerebral arteriovenous malformation characterized by a plexiform nidus with an afferent arterial pedicle and a draining vein.63
Pulmonary arteriovenous fistulae set the stage for paradoxical emboli, stroke, and brain abscess (see Figure 30-6).18,32,63–68 Intracranial malformations induce grand mal seizures, which can be fatal.69 Sudden death results from massive intrapulmonary hemorrhage and massive hemothorax.18,24,58 A 41-year-old woman whose case was reported in 1906 died of intractable epistaxes.70 Platypnea-orthodeoxia has been described with pulmonary arteriovenous fistula and a patent foramen ovale.71



