Chapter 23 Congenital Aneurysms of the Sinuses of Valsalva
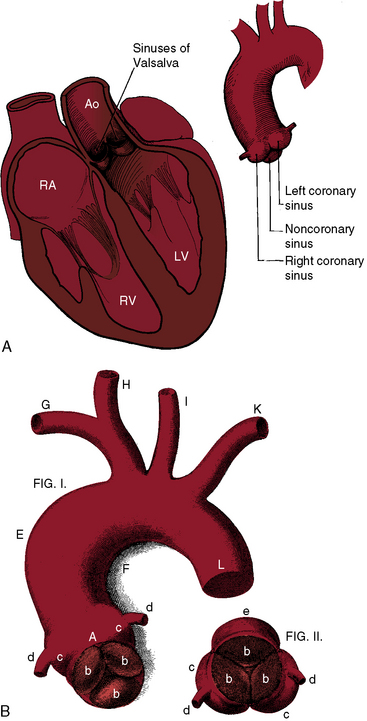
Antonio Maria Valsalva, anatomist and pathologist, was born in 1666 in the historic Emilia-Romagna region of northern Italy. The sinuses that bear Valsalva’s name consist of three small outpouchings in the wall of the aorta immediately above the attachments of each aortic cusp (Figure 23-1). In 1839, James Hope1 published an account of a ruptured congenital aneurysm of a sinus of Valsalva, “a case of aneurysmal pouch of the aorta bursting into the right ventricle.” A year later, John Thurnam2 expanded Hope’s report by adding examples of unruptured aortic sinus aneurysms and by naming the sinuses according to their relationship to the coronary arteries as the right coronary sinus, the left coronary sinus, and the noncoronary sinus (see Figure 23-1). These designations appeared in Quain’s Elements of Anatomy3 and remain in use today.4
Aneurysms of the sinuses of Valsalva account for 1% of congenital anomalies of the heart and circulation.5 The aneurysms tend to be single, although exceptionally, more than one sinus is involved.6,7 An aneurysm may arise from each sinus of a bicuspid aortic valve,6,8 from each sinus of a trileaflet aortic valve,7 and rarely, from a quadricuspid aortic valve.9
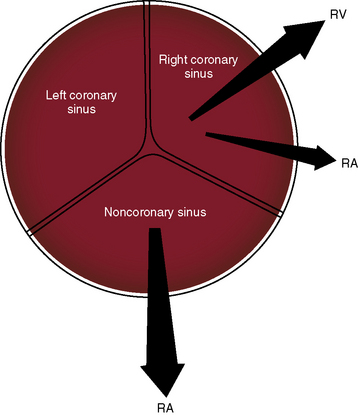
The anatomic relationship of the sinuses of Valsalva to adjacent structures determines the site into which a given congenital aneurysm ruptures.4 Ninety percent to 95% originate in the right or noncoronary sinus and project into the right ventricle or right atrium, and less than 5% originate in the left coronary sinus (Figure 23-2).4,10,11 Those that arise in the noncoronary sinus almost always rupture into the right atrium (see Figure 23-2), and those that arise in the right coronary sinus rupture into the right ventricle or occasionally into the right atrium (see Figure 23-2).4 Rarely, rupture is into the pulmonary artery,10,12 left ventricle,4 left atrium,4 or pericardial space.4,13 Also rarely, a sinus aneurysm dissects into the interventricular septum, where it remains unruptured or perforates and ruptures into the left or right ventricle.5,14–16 A congenital etiology is questionable when an aneurysm originates in the left coronary sinus and ruptures into the left side of heart.4
A sinus of Valsalva aneurysm can cause aortic regurgitation by interfering with aortic leaflet coaptation, can enter the right atrium and cause tricuspid regurgitation,17 or can enter the right ventricular outflow tract and cause subpulmonary obstruction. A congenital aortic sinus aneurysm that is the site of infective endocarditis can be difficult to distinguish from aortic valve infective endocarditis that caused the aortic sinus to perforate.4,18–20 A large unruptured aneurysm can compress the superior vena cava, the right atrium, the right ventricle,21 or a coronary artery.
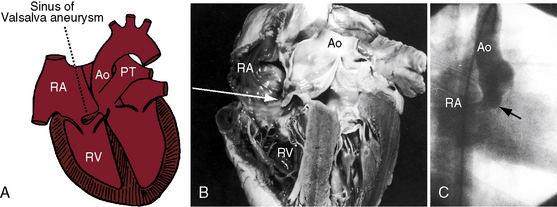
A congenital sinus of Valsalva aneurysm begins as a blind pouch or diverticulum at a localized site in an aortic sinus and then protrudes as a finger-like or nipple-like projection that ruptures at its tip (Figure 23-3).4,22,23 The fundamental histologic fault responsible for a coronary sinus aneurysm is discontinuity of the elastic layer in the aortic media at the juncture between the ascending aorta and aortic valve annulus, which sets the stage for avulsion and aneurysm formation.23,24 The histologic fault is present at birth, but with rare exception, the aneurysm is not.18,25,26 Marfan syndrome is associated with dilation of the ascending aorta and the sinuses of Valsalva, but dissection or rupture is in the ascending aorta, not in the sinuses.27 An aorticocameral communication is a tortuous channel that originates the ascending aorta above the left sinus of Valsalva and terminates in the right atrium without involving the aortic sinuses.28
The physiologic consequences of rupture depend on three factors: 1, the amount of blood flowing through the rupture; 2, the rapidity with which the rupture develops; and 3, the chamber that receives the rupture. Irrespective of the right-sided receiving site, shunted blood must flow through the pulmonary circulation, the left atrium, and the left ventricle before returning to the aorta. When the right atrium receives the rupture, all four cardiac chambers are volume overloaded. A sudden large rupture provokes congestive failure because the heart cannot adapt rapidly to the acute hemodynamic burden. Conversely, small insidious perforations initially go unnoticed (Figure 23-4). Deformity of aortic cusps caused by a ruptured or unruptured aneurysm causes regurgitation through the valve (Figure 23-5), and rupture of a sinus aneurysm into the left ventricle causes regurgitation through the rupture.29 Aneurysms that originate in the right sinus of Valsalva are typically associated with a supracristal ventricular septal defect (see Figure 23-5).4,23,30–32
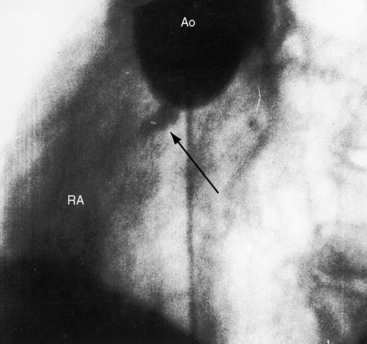
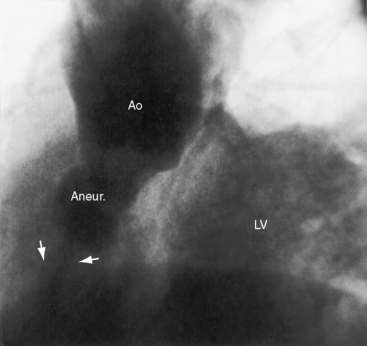
Figure 23-5 Aortogram from a 31-year-old woman with an asymptomatic restrictive ventricular septal defect and mild to moderate aortic regurgitation. Sudden dyspnea, orthopnea, and a coarse continuous murmur were caused by rupture of an aneurysm (Aneur., arrows) of the right sinus of Valsalva into the right ventricle. The left ventricle (LV) visualized because of aortic regurgitation. The echocardiogram is shown in Figure 23-14. (Ao = aorta.)
Unruptured congenital sinus of Valsalva aneurysms were recognized by Thurnam (see previous).2 Before the advent of echocardiography, approximately 20% of unruptured aneurysms were chance findings at necropsy or at cardiac surgery.33 However, occult unruptured congenital aortic sinus aneurysms are now readily imaged, even in older adults (see Figure 23-17).28,34 An unruptured aneurysm can compress a proximal coronary artery or can dissect into the ventricular septum and cause complete heart block.34 Protrusion of an aneurysm into the left ventricle is occasionally responsible for aortic regurgitation (see previous),29 less commonly for obstruction to left ventricular outflow.

History
Ruptured aortic sinus aneurysms typically announce themselves in young males after puberty but before age 30 years. The male:female ratio is as high as 4:1.22 Rupture rarely occurs in infancy or early childhood25,26,35 or as late as the seventh decade36,37 and rarely occurs during pregnancy.38 The average age of rupture was 34 years in one large series, with an age range of 11 years to 67 years.36 An unruptured congenital aneurysm of the right coronary sinus was an incidental necropsy finding in a 82-year-old man,33 and an 85-year-old man came to attention because an occult unruptured aortic sinus aneurysm in the right ventricular outflow tract caused a to-and-fro murmur (see Figure 23-17). Death from congestive heart failure typically occurs within a year after rupture.36 Sudden death follows perforation into the pericardium, and syncope and sudden death are occasional sequelae of complete heart block caused by a ruptured15 or unruptured34 aneurysm that dissects into the base of the ventricular septum.15,39 Conversely, long survival sometimes follows a small slowly progressive perforation (see Figure 23-4). One such individual lived for 30 years, and another lived for 17 years;40 a 65-year-old man died of gastric carcinoma 10 years after rupture,37 and rupture in infancy was followed by surgical repair 15 years later. Small perforations come to attention because of a continuous murmur (see Figure 23-4),41 because of a diastolic murmur caused by aortic regurgitation, because of infective endocarditis,4,19 or during a diagnostic study for ventricular septal defect.42 A large unruptured saccular aneurysm filled with laminated thrombus came to light because of a prominent paracardiac density on a routine chest x-ray, and another unruptured aneurysm announced itself with cerebral and retinal emboli.43 Compression of a coronary artery by an unruptured aneurysm is a rare cause of angina pectoris or myocardial infarction (see previous). In 1957, a 27-year-old soldier with a large acute rupture underwent the first successful surgical repair with a polyvinyl prosthesis shaped as a golf tee. Three decades later, the patient had dramatic reperforation (see second case history subsequent).44
Congenital sinus of Valsalva aneurysms come to attention because of the acute development of a large perforation, gradual progression of a small perforation, or an asymptomatic or symptomatic unruptured aneurysm. An large acute rupture is announced by the dramatic onset of severe retrosternal or upper abdominal pain and intractable dyspnea.31,36 The rupture often but not necessarily follows physical stress. The acute symptoms last for hours or days, sometimes subsiding gradually, leaving the patient’s condition temporarily improved, but congestive heart failure appears and progresses relentlessly. The following case histories are illustrative.
The first history describes a 45-year-old truck driver whose work included strenuous lifting of 50-lb to 100-lb sacks of plaster.31 He was in good health until 3 weeks before an alarming experience. While carrying a 100-lb sack, he suddenly became “out of breath” and fell to the floor. A raw sensation radiated from the epigastrium to the base of the neck. Despite severe weakness and shortness of breath, he carried 20 more sacks before consulting a doctor. When seen by the authors, he was relatively asymptomatic.
The initial pain is believed to be related to the rupture itself. Occasionally, the aneurysm compresses a coronary artery, so symptoms of myocardial ischemia or infarction coexist.45 Rupture may be announced by acute dyspnea rather than pain, or mild chest pain may occur for weeks before the onset of dyspnea and tightness in the upper abdomen. If a patient with a ventricular septal defect suddenly develops chest pain, dyspnea, and a continuous murmur, the reason is likely to be rupture of a coexisting aortic sinus aneurysm (see Figure 23-5; see previous).
Small insidious perforations that initially progress gradually go unnoticed (see Figures 23-4 and 23-16). Mild dyspnea without pain sometimes precedes congestive heart failure by months or years.17 Patients sometines present during a relatively asymptomatic interval with a continuous murmur mistaken for patent ductus arteriosus.
Congenital aortic sinus aneurysms usually go unrecognized until they rupture.33 However, unruptured aneurysms can manifest themselves with a to-and-fro murmur from flow in and out of the intact aneurysmal pouch (see Figure 23-17), with the murmur of tricuspid regurgitation, with a midsystolic murmur of right ventricular outflow obstruction, with the pain of myocardial ischemia from coronary artery compression, with aortic regurgitation–caused malapposition of aortic cusps,29 with superior vena caval obstruction,21 with a paracardiac mass in the chest x-ray, with systemic emboli,43 with complete heart block, with syncope, or with sudden death.15



