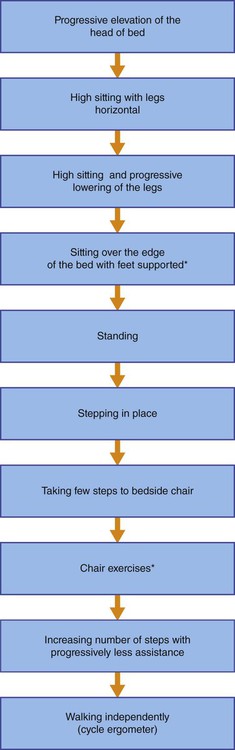
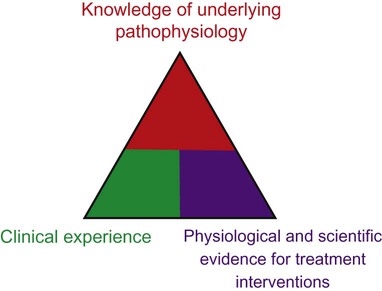
The thrust toward evidence-based practice in health care and the development of conceptual bases for practice have had major implications for cardiovascular and pulmonary physical therapy in the ICU.1–4 Superior knowledge of cardiovascular and pulmonary physiology, pathophysiology, pharmacology, multisystem dysfunction and its medical management, and ICU equipment and changing technology is essential. Clinical decision making in the ICU and rational management of patients is based on a tripod approach: knowledge of the underlying pathophysiology and basis for general care; knowledge of the physiological and scientific evidence for treatment interventions; and clinical reasoning and decision making in prioritizing treatments, prescribing their parameters, and performing serial evaluation to assess outcomes and further modify treatment (Figure 33-1). High-quality care is a function of these three areas of knowledge and expertise. Evidence-based practice and excellent problem-solving ability will optimize outcomes5 and maximize the benefit-to-risk ratio of cardiovascular and pulmonary physical therapy interventions. Effective clinical decision making and practice in the ICU demand specialized expertise and skill, including advanced, state-of-the-art knowledge in cardiovascular and pulmonary and multisystem physiology and pathophysiology and in medical, surgical, nursing, and pharmacological management (Box 33-1). Physical therapists in the ICU need to be first-rate diagnosticians and observers. Given the multitude of factors that contribute to impaired oxygen transport,6 the physical therapist needs to analyze these to define the patient’s specific oxygen transport deficits and problems. Optimizing oxygen delivery in the patient who is critically ill7 by exploiting noninvasive interventions is the priority. Box 33-1 Specialized Expertise and Skill of the Intensive Care Unit Physical Therapist 1. Return the patient to his or her premorbid functional level or a higher level if possible 2. Reduce complications, morbidity, premature mortality, and length of ICU and overall hospital stay Many elements of the assessment of patients in the ICU are comparable to those for patients with acute conditions who are not critically ill but require respiratory support and mechanical ventilation (see Chapter 44). The primary difference is that for patients in the ICU the adequacy of the steps in the oxygen transport pathway are monitored closely, and the status and function of multiple organ systems are monitored in a serial (repeated at regular or judicious intervals) manner to observe trends over time so that treatment modifications can be titrated to the patient’s responses. Serial vital signs including pain and distress are recorded along with arousal and cognitive status, neuromuscular status, musculoskeletal status, and functional mobility. Assessment of functional mobility ranges from the smallest movement to walking (see Figure 33-2 and Box 33-4). Often it includes bed mobility, transfers to chair, and walking, which may require assistive devices. Related laboratory investigations are noted, including the electrocardiogram (ECG), radiographs, scans, blood work, blood sugar level, and fluid and electrolyte balance, and are followed closely to quickly detect improvement or deterioration so that treatment can be correspondingly modified. Mechanical ventilation and its modes and parameters are described in Chapter 44. The ventilator settings including the fraction of inspired oxygen (FIO2) are important indicators of changes in the patient’s status and therefore must be included in the assessment and recorded at each treatment. Similarly, changes in FIO2 are important outcomes and indicators of treatment response. This information is used collectively in clinical decision making before, during, and after weaning from mechanical ventilation. In patients who are medically stable, invasive mechanical ventilation is titrated judiciously to ensure that the patient is initiating breaths as much as possible, which facilitates weaning. Depending on the patient’s response to ventilation, however, sedation and neuromuscular blockade may be indicated. These interventions limit the patient’s capacity to cooperate fully with treatment. Breathing patterns imposed by the mode of mechanical ventilation influence venous return and aortic pressures8; thus mobilization needs to be prescribed accordingly. Furthermore, weaning patients with chronic obstructive pulmonary disease (COPD) and neuromuscular conditions is complicated by respiratory muscle weakness and fatigue (see Chapter 26), which may indicate respiratory muscle training or rest. Because of these challenges, weaning necessitates close cooperation and coordination within the team to maximize weaning success. As for patients who are not critically ill, the assessment data are evaluated, problems and diagnoses made, and interventions prescribed based on the patient’s needs and goals. Physical therapy has a prominent role in the management of patients who are on mechanical ventilation.9,10 With each treatment, the responses are reviewed and prescription parameters of the interventions are refined to progress the patient Hospitalization, particularly in the ICU, is associated with a considerable reduction in mobility (i.e., loss of exercise stimulus) and recumbency (i.e., loss of gravitational stimulus) (see Chapters 18 and 20).11–13 These two factors are essential for normal oxygen transport; thus their removal has dire consequences for the patient with or without cardiovascular and pulmonary dysfunction. In terms of a physiological hierarchy of treatment interventions (see Chapter 17), exploiting the physiological effects of acute mobilization, upright positioning, and their combination is the most physiologically justifiable primary intervention to maximize oxygen transport and prevent its impairment in patients who are critically ill. Recumbency is nonphysiological; it is a position in which, all too often, most patients are injudiciously confined. Changing the position of the body from erect to supine positions results in significant physiological changes that may jeopardize the patient’s already compromised or threatened oxygen transport system (Box 33-2) (see Chapter 20). Box 33-2 Physiological Changes When Changing from the Upright to the Supine Position Physical therapy interventions in the ICU (see Chapter 17 and Part III) are more specifically geared toward the status of each organ system, taking into consideration the pathophysiological basis for the patient’s signs and symptoms, the rationale for each intervention, and the physiological and scientific evidence supporting the effectiveness of the intervention.14 Physical therapy provides both prophylactic and therapeutic interventions for the patient in the ICU. Conservative, noninvasive measures constitute initial treatments of choice to avert or delay the need for additional invasive monitoring and treatment including supplemental oxygen, pharmacological agents, and the need for intubation and mechanical ventilation. The physical therapist aims to avoid, reduce, or postpone for as long as possible the need for respiratory support. Even if the patient is mechanically ventilated, maintaining some level of spontaneous breathing, no matter how minimal, is associated with improved oxygenation and outcomes.15 In addition, the physical therapist helps to prevent the multitude of side effects of restricted mobility and recumbency during bed rest. A summary of general information required before treatment of the patient in the ICU is presented in Box 33-3. This provides the basis for establishing a patient’s readiness to be mobilized and the progressive steps for doing so (Box 33-4 and Figure 33-2). Box 33-3 General Information Required before Treatment of the Patient in the Intensive Care Unit Box 33-4 Guiding Principles for Mobilizing Patients in the Intensive Care Unit Based on a multisystem assessment and discussion with the team: Maximizing function refers to maximizing the capacity to participate in one’s life roles and associated activities. This necessitates promotion of optimal physiological functioning at an organ system level, as well as promoting maximal functioning of the patient as a whole. In critical care, primary goals related to function optimization are initially focused on cardiovascular and pulmonary function. With improvement in oxygen transport, increased attention is given to optimal functioning of the patient with respect to self-care, self-positioning, sitting up, and walking. General physical therapy goals related to function optimization are shown in Box 33-5. Outcomes can be tracked objectively by recording the length of time a patient sits over the edge of the bed, sits in a chair at bedside, stands, and walks. Also, the weight a patient lifts as well as the number of repetitions and sets he or she performs can be readily quantified.
Comprehensive Management of Individuals in the Intensive Care Unit
Specialized Expertise of the Intensive Care Unit Physical Therapist
 Detailed, comprehensive knowledge of cardiopulmonary physiology and pathophysiology and pharmacology.
Detailed, comprehensive knowledge of cardiopulmonary physiology and pathophysiology and pharmacology.
 Ability to practice effectively under pressure and in congested, suboptimal working conditions.
Ability to practice effectively under pressure and in congested, suboptimal working conditions.
 Knowledge regarding the roles of all team members.
Knowledge regarding the roles of all team members.
 Superior communication skills (e.g., ability to work cooperatively with other members of the ICU team [Figure 33-3] and give verbal presentations and discuss patients at rounds).
Superior communication skills (e.g., ability to work cooperatively with other members of the ICU team [Figure 33-3] and give verbal presentations and discuss patients at rounds).
Goals and General Basis of Management
Restricted Mobility and Recumbency
 Cephalad displacement of the visceral contents and diaphragm
Cephalad displacement of the visceral contents and diaphragm
 Compression of the dependent lung fields
Compression of the dependent lung fields
 Cephalad fluid shift to the central circulation
Cephalad fluid shift to the central circulation
 Increased stroke volume and cardiac output and over days a reduction caused by renal compensation
Increased stroke volume and cardiac output and over days a reduction caused by renal compensation
 Decreased functional residual capacity
Decreased functional residual capacity
 Decreased forced expiratory volumes
Decreased forced expiratory volumes
 Increased closing volumes of small airways
Increased closing volumes of small airways
 Increased restriction of chest wall and decreased diaphragmatic excursion
Increased restriction of chest wall and decreased diaphragmatic excursion
 Decreased pulmonary and chest wall compliance
Decreased pulmonary and chest wall compliance
 Decreased arterial oxygen levels
Decreased arterial oxygen levels
 Increased preload, afterload, and myocardial work
Increased preload, afterload, and myocardial work
 Decreased myocardial efficiency
Decreased myocardial efficiency
 Decreased sympathetic stimulation and decreased peripheral vascular resistance
Decreased sympathetic stimulation and decreased peripheral vascular resistance
Specificity of Cardiovascular and Pulmonary Physical Therapy
 Knowledge of patient’s life roles and related activities for optimal return to daily life
Knowledge of patient’s life roles and related activities for optimal return to daily life
 Medical and surgical histories
Medical and surgical histories
 General multisystem assessment findings
General multisystem assessment findings
 Hydration and nutritional status: deficiencies, obesity, or asthenia
Hydration and nutritional status: deficiencies, obesity, or asthenia
 Time of onset and course of present condition
Time of onset and course of present condition
 Existing or potential medical instability
Existing or potential medical instability
 Indications or necessity for intubation and mechanical ventilation
Indications or necessity for intubation and mechanical ventilation
 Mode and parameters of mechanical ventilation
Mode and parameters of mechanical ventilation
 Invasive monitoring, lines, leads, and catheters
Invasive monitoring, lines, leads, and catheters
 Existence of or potential for complications and multiorgan system failure
Existence of or potential for complications and multiorgan system failure
 Presence of elevated intracranial pressure (ICP) and the need for ICP monitoring
Presence of elevated intracranial pressure (ICP) and the need for ICP monitoring
 Risk or presence and site(s) of infection
Risk or presence and site(s) of infection
 Quality of sleep and rest periods
Quality of sleep and rest periods
 Nutritional support during intensive care unit stay
Nutritional support during intensive care unit stay
 Determine the patient’s readiness for mobilization—that is, perform multisystem assessment including arousal, medications, lines and leads, mechanical ventilation and respiratory support; responses to gravitational and mobilization challenge tests; contraindications and precautions and clearance by team.
Determine the patient’s readiness for mobilization—that is, perform multisystem assessment including arousal, medications, lines and leads, mechanical ventilation and respiratory support; responses to gravitational and mobilization challenge tests; contraindications and precautions and clearance by team.
 Prescribe the parameters of the gravitational and mobilization stimuli (types of mobilization and exercise, their intensities, duration, and frequencies) by titrating them to the patient’s immediate and longer term responses (see Fig 33-2 for progression of mobilization). Principles for progressing the mobilization stimulus:
Prescribe the parameters of the gravitational and mobilization stimuli (types of mobilization and exercise, their intensities, duration, and frequencies) by titrating them to the patient’s immediate and longer term responses (see Fig 33-2 for progression of mobilization). Principles for progressing the mobilization stimulus:
 Progression to successive steps is based on the patient’s responses.
Progression to successive steps is based on the patient’s responses.
 The patient is reassessed before each bout of mobilization and evaluated throughout and afterward.
The patient is reassessed before each bout of mobilization and evaluated throughout and afterward.
 Increased intensity. Increase is commensurate with reduction of support and assistance, and increased duration to increase volume of exercise overall, and with improvement—that is, the patient tolerates greater gravitational stress and exercise stress with reduced physiologic demands within therapeutic and safe limits)
Increased intensity. Increase is commensurate with reduction of support and assistance, and increased duration to increase volume of exercise overall, and with improvement—that is, the patient tolerates greater gravitational stress and exercise stress with reduced physiologic demands within therapeutic and safe limits)
Maximizing Function
Comprehensive Management of Individuals in the Intensive Care Unit