aSome material was contributed by William Grossman and Donald Baim in their role as authors of this chapter in prior editions.
The risk of complications is inherent to any medical treatment, irrespective of its invasive nature. In particular, given that cardiac catheterization involves inserting foreign objects (i.e., cardiac catheters) into the circulatory system and the use of catheters and devices to diagnose and treat vascular and structural abnormalities, it is not surprising that cardiac catheterization can be associated with a variety of complications. These complications range from minor problems with no longterm sequelae (e.g., transient bradycardia during coronary contrast injection) to major problems (e.g., cardiac perforation, abrupt closure of a coronary artery during percutaneous coronary intervention [PCI]) that may require immediate surgical attention, to major and irreversible damage (e.g., stroke, myocardial infarction, renal failure, or death). Fortunately, the risk of producing a major complication during most procedure types is generally below 1%, a level at which the risk-benefit ratio still favors the performance of cardiac catheterization to investigate or treat cardiac disorders that are themselves life threatening or symptom limiting. In this chapter, we outline general complications that are common to most procedures. For additional information on less common complications, and on corresponding prevention and bailout techniques, our readers are referred to individual chapters in this textbook and to other textbooks that have been written on this topic.1
OVERVIEW
The determinants of the risk for sustaining a complication during an invasive procedure include the clinical characteristics of the patient, equipment limitations, and operator experience. The risk thus varies widely depending on demographics (age, gender), the cardiac anatomy (left main coronary artery disease, severe aortic stenosis, diminished left ventricular function), and the clinical situation (unstable angina, acute myocardial infarction, cardiogenic shock). Other variations in risk are based on the type of procedure being performed (diagnostic catheterization, coronary intervention, and so on) and to some extent on the experience and familiarity of the operator with that particular procedure.
By considering all these factors, the physicians and support staff can arrive at a fairly accurate estimate of the level of risk entailed in any given procedure. Familiarity with those risks can be of immeasurable value in the following: (a) anticipating increased risks of complications; (b) taking extra precautions to avoid them (e.g., placing a prophylactic pacemaker in a patient prior to rotational atherectomy of a right coronary artery lesion); (c) promptly recognizing complications when they occur (e.g., perforation of the right atrium during a transseptal puncture); and (d) taking corrective and potentially lifesaving action (e.g., pericardiocentesis for perforation-induced tamponade).
Before proceeding with any procedure, the details of the planned procedure and its anticipated risks must be discussed candidly with the patient and family.2 This discussion should include which specific procedures are planned, what benefits are hoped for, the attendant risks and their probabilities, and how the risks and benefits of the planned procedure compare with those of any possible alternatives (e.g., coronary artery bypass graft surgery instead of percutaneous coronary intervention). By covering these cornerstones of informed consent clearly and candidly, the patient and family will be realistically prepared should a complication occur. Such a discussion should be documented in the patient’s chart, and that documentation should specify the type of procedure that is planned, the potential major complications, and their estimated risk of occurrence (see also Chapter 1). If a significant major complication does occur, the patient and family should be informed of the same as soon as the procedure has been completed (or when a delayed complication occurs, as soon as it is recognized). This discussion should describe the nature of the complication (without placing blame on anyone), indicate whether any long-term consequences are expected, and outline what corrective actions have been and will continue to be pursued. The catheterizing physician should also continue daily inpatient follow-up visits to any patient who has sustained a significant complication, because a patient’s feeling of abandonment by an uncaring physician tends to foster a desire for retribution (i.e., a malpractice suit).
Therefore, all individuals performing cardiac catheterization should thoroughly know the potential complications of the procedures they perform, as detailed in this and other chapters. In addition, the catheterization laboratory director should collect information about the frequency of these complications on at least a yearly basis and should review those data with the physician staff to identify where the laboratory as a whole (or an individual operator) is performing below expected standards. The types of complications that are routinely tracked in this process are shown in Table 4.1. This type of data collection, analysis (including breakdown by procedure type and by individual operator), reporting, and subsequent adjustment in laboratory policy and procedures2 is one of the most important jobs of any catheterization laboratory director and has now become a reporting requirement in several states.
Table 4.1 Performance Measures and Quality Metrics Currently Reported in the Cath PCI Registry Executive Summary, American College of Cardiology Foundation National Cardiovascular Data Registry. All Hospitals ending 2010Q2.(https://www.ncdr.com/webncdr/cathpci/home/sample-reports). (Access Date 05/31/2013).
Incidence of nonobstructive CAD (elective patients only)
Diagnostic Cath Outcomes Metrics
Vascular access site injury requiring treatment or major bleeding
Utilization Metrics
Median postprocedure length of stay (in days) for PCI patients with STEMI
Median postprocedure length of stay (in days) for PCI patients with no STEMI
Data Quality Metrics
Creatinine assessed pre- and post-PCI procedure
Test Metrics
Test Metric: Transfusion of whole blood or RBCs
Test Data Quality Metric: Biomarkers assessed post-PCI for elective inpatients
DEATH
Death as a Complication of Diagnostic Catheterization
Death as a complication of diagnostic catheterization has declined progressively over the last 30 years. Whereas a 1% mortality was seen with diagnostic catheterization in the 1960s,3 the first Society for Cardiac Angiography registry of 53,581 diagnostic catheterizations performed in 1979-1981 showed a 0.14% procedure-related mortality.4 By the second registry of 222,553 patients catheterized in 1984-1987,5 procedure-related mortality for diagnostic catheterization had fallen further, to 0.1% (i.e., 1 in 1,000). This small reduction in mortality, however, belies the fact that the second registry included many more patients who fell into a high-risk subgroup for the procedure. Based on variables identified from the 218 deaths in the second registry (age older than 60 years, New York Heart Association (NYHA) functional class IV, left ventricular ejection fraction <30%, or left main disease), the mortality for such patients fell by half between the first and second registry.6 A third registry of 58,332 patients studied in 1990 showed an even lower overall mortality of 0.08%, with a 1.5% incidence of any major complication.7 A number of baseline variables (including NYHA class, multivessel disease, congestive heart failure, and renal insufficiency) were identified in this registry, whose presence predicted an up to eightfold increase in major complication rates (from 0.3% in patients with none of these factors to 2.5%).8 Several of the major factors are discussed below.
Left Main Disease
Although there has been a progressive reduction in the overall mortality of diagnostic cardiac catheterization over the last 25 years, patients with severe left main coronary disease remain at increased risk. Their mortality was 6% in the 1976 report by Bourassa,9 and 2.8% in the study by Boehrer and others performed between 1978 and 1992 (compared with a mortality of 0.13% in patients without such disease).10 Although the mortality of such patients had fallen to 0.86% in the first Society for Cardiac Angiography registry, this was still more than 20 times higher than the 0.03% mortality seen in patients with single-vessel disease.4
Because roughly 7% of patients undergoing coronary angiography have significant left main disease, the protocol used for coronary angiography (see Chapter 15) should always begin with careful catheter entry into the left coronary ostium to facilitate early recognition of ostial left main disease through catheter pressure damping or performance of a test “puff” immediately after engagement. Even without these early warnings of left main disease, we routinely perform the first left coronary injection in the right anterior oblique (RAO) projection with caudal angulation to screen for mid and distal left main disease and get the maximal anatomic information on the first injection. If ostial left main stenosis is suspected, a straight anterior (AP) injection may be performed. If severe left main disease is present, the only other left coronary injection needed is an RAO projection with cranial angulation (to see the left anterior descending and its diagonal branches). If angiography shows a borderline lesion (30% to 50%), additional diagnostics including intravascular ultrasound (IVUS; Chapter 25) or pressure wire (Chapter 24) can be performed after completing diagnostic coronary angiography to inform the subsequent management decision. However, performing a large number of superfluous contrast injections in a patient with a critical left main disease offers little more in the way of important anatomical information and increases the risk of triggering the vicious cycle of ischemia/hypotension/more ischemia that may lead to irreversible collapse.
Careful attention to all other aspects of technique is essential, since even an otherwise minor complication (e.g., a vasovagal reaction or arrhythmia) may have fatal consequences in this situation. If a patient with severe left main disease exhibits any significant instability during the procedure, we usually opt to place an intraaortic balloon pump (see Chapter 27) and arrange for prompt coronary artery bypass graft surgery. When the hemodynamics are markedly compromised and the patient is a poor surgical candidate, emergency coronary stenting can be performed if a trained operator and the necessary equipment are available (see Chapters 27 and 28). A similar consideration regarding the use of hemodynamic support applies to any patient with an unstable ischemic syndrome or acute myocardial infarction who behaves in a brittle fashion under the stresses of catheter placement and contrast injection.
Left Ventricular Dysfunction
Patients with cardiogenic shock in the setting of acute myocardial infarction or severe chronic left ventricular dysfunction (ejection fraction <30%) also have a several-fold increased risk of procedural morbidity and mortality,5 particularly when reduction in ejection fraction is associated with a baseline pulmonary capillary wedge pressure >25 mmHg and a systolic arterial pressure <100 mmHg. An effort should be made to bring such congestive heart failure under control before cardiac catheterization is attempted.
Although right heart catheterization is no longer routine (see Chapter 6), it should be performed before angiography in a patient with poor ejection fraction, because it provides valuable data about baseline hemodynamic status and allows ongoing monitoring of pulmonary artery pressure as an early warning about hemodynamic decompensation before frank pulmonary edema ensues. If the baseline pulmonary capillary wedge pressure is >30 mmHg, every effort should be made to improve hemodynamic status before angiography is attempted. This may entail administration of a potent intravenous diuretic (furosemide), supplemental oxygen, a vasodilator (intravenous nitroglycerine or sodium nitroprusside) when the mean arterial pressure is >65 mmHg, or a positive inotrope (dobutamine, milrinone) when the mean arterial pressure is <65 mmHg, or when severe congestive heart failure hemodynamics persist despite vasodilator treatment (see below). When frank cardiogenic shock is present or develops during a cardiac catheterization, prompt placement of an intraaortic balloon pump or of alternative percutaneous left ventricular assist devices in the contralateral groin may be required to get the patient safely though the procedure (see Chapter 27). Low-osmolar contrast agents produce less myocardial depression than traditional high-osmolar agents. They have replaced high-osmolar contrast agents for the performance of coronary and vascular angiography and they have greatly enhanced our ability to perform necessary angiography without precipitating hemodynamic decompensation in such unstable patients (see Chapter 2).
Valvular Heart Disease
Despite the preponderance of coronary artery disease as the indication for diagnostic cardiac catheterization patients with severe valvular heart disease are also at increased risk for dying during cardiac catheterization. The VA Cooperative Study on Valvular Heart Disease11 showed a 0.2% mortality among 1,559 preoperative catheterizations performed in patients with valvular heart disease, with one death in a patient with mitral regurgitation and two deaths in patients with aortic stenosis. With current noninvasive methods for assessing the severity of valvular lesions, there has been debate about whether it is necessary to cross severely stenotic valves in the course of preoperative cardiac catheterization.12 According to the most recent ACC/AHA update to the 2006 Guidelines for the Management of Patients with Valvular Heart Disease, cardiac catheterization is not recommended for the assessment of severity of aortic stenosis before aortic valve replacement “when noninvasive tests are adequate and concordant with clinical findings (Level of Evidence: C).”13
Prior Coronary Artery Bypass Graft Surgery
Patients who have previously undergone coronary bypass surgery make up a growing subgroup of diagnostic and interventional catheterizations. They are typically 5 years older, have more diffuse coronary and generalized atherosclerosis, worse left ventricular function, and require a lengthier and more complex procedure to image both native coronary arteries and all grafts. Despite these adverse risk factors, the Post CABG Trial14 looked at 2,635 diagnostic angiograms performed in stable patients and found 0% mortality, with major complications in 0.7% (myocardial infarction 0.08%, stroke 0.19%, vascular trauma requiring transfusion or surgery 0.4%).
Pediatric Patients
Pediatric patients may be at higher risk (see Chapter 9). One review of 4,952 patients (median age 2.9 years) studied at the
Hospital for Sick Children in Toronto15 found a mortality of 1.2% confined to patients younger than age 5 years (half in critically ill neonates <30 days of age). Although the risk was lower for diagnostic than for electrophysiologic or interventional procedures, there were three deaths (0.1%) among the 3,149 diagnostic procedures.
Death in the Course of an Interventional Procedure
Because they involve the use of more aggressive catheters, superselective cannulation of diseased coronary arteries, and brief interruption of coronary or even systemic flow (see Chapter 28), interventional procedures tend to carry higher mortality than purely diagnostic catheterizations. In the first 1,500-patient coronary angioplasty registry sponsored by the National Heart, Lung, and Blood Institute (NHLBI) from 1979 to 1982, the mortality of elective angioplasty was 1.1%.16 This was relatively unchanged at 1.0% in the second NHLBI registry of 1,802 patients treated at 15 centers between 1984 and 1987, mainly because the second registry included more patients with adverse features (advanced age, poor ventricular function, multivessel disease, prior bypass surgery, and so on).17 In fact, the mortality for single-vessel procedures fell from 1.3% to 0.2% between the first and second registry.
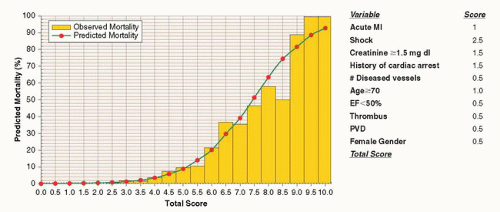
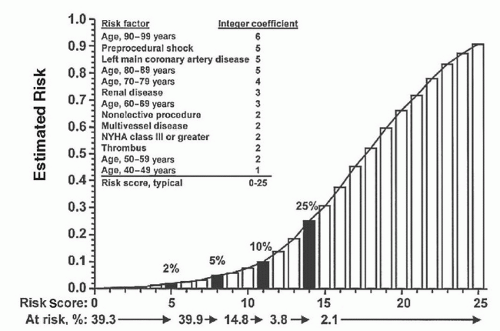
With the introduction of newer devices (e.g., stents, atherectomy, laser) to treat high-risk lesions preemptively or reverse abrupt closure following attempted conventional balloon angioplasty, the overall mortality for elective coronary intervention has fallen further (Chapter 28), but the extension of intervention to other high-risk subsets, including patients with acute myocardial infarction undergoing primary angioplasty, has kept overall mortality close to 1%18,19— roughly 10-fold higher than purely diagnostic catheterization (i.e., 1% vs. 0.1%). Several multivariable models that predict procedural mortality have been developed based on age, ejection fraction, treatment for acute myocardial infarction/shock, urgent/emergent priority, and so on18, 19, 20, 21, 22, 23, 24 (see also Chapter 28 and 30). In general, there is a wide variation in risk of death in the course of coronary intervention—based on patient comorbidities, clinical indication, and procedure type. While an “average” risk can be quoted to “average” patients, patients with one or more adverse risk factors should be told candidly during the informed consent process that their expected risks are higher than these averages (Figures 4.1 and 4.2). A similar approach can be used when discussing prognosis following PCI for acute myocardial infarction or cardiogenic shock.
MYOCARDIAL INFARCTION
Although transient myocardial ischemia is relatively common during diagnostic catheterization and occurs routinely during coronary intervention, myocardial infarction is an uncommon but important complication of diagnostic cardiac catheterization. In the late 1970s, data from the Coronary Artery Surgery Study showed a myocardial infarction rate of 0.25% for coronary angiography.25 In the first, second, and third registries conducted by the Society for Cardiac Angiography and Interventions,4,5,7 the risk of myocardial infarction fell progressively, from 0.07%, to 0.06%, to 0.05%. However, the risk of precipitating myocardial infarction during diagnostic catheterization is clearly influenced by patient-related factors that include the extent of coronary disease (0.06% for single-vessel disease, 0.08% for triplevessel disease, and 0.17% for left main disease),5 the clinical indication (e.g., unstable angina or recent subendocardial infarction), and the presence of insulin-dependent diabetes. The progressive reduction in overall risk of myocardial infarction since the 1970s likely reflects greater attention to procedure technique including catheter flushing, pressure damping, and management of the arterial sheath during catheters exchange—all nuances that are now considered integral parts of coronary angiography (see Chapter 15). However, it should also be pointed out that this decrease might also reflect better patient preparation with beta blockade, use of preprocedure aspirin and preprocedure statins, as well as ready availability of ad hoc PCI for unstable patients with anatomically suitable disease.
Figure 4.1 Example of a risk prediction rule for percutaneous coronary intervention (PCI) mortality. For the estimation of risk, the total score can be calculated by adding individual scores if the comorbidity is present. For # of diseased vessels, a score of 0.5 should be added for each major epicardial vessel that has >70% stenosis. The total score can then be transferred to the horizontal axis of the plot, and the corresponding probability of death can be estimated on the vertical axis. Scores <2.5 are associated with a risk of death <0.8%, while scores >7 are associated with a risk of death >40%. (Reproduced with permission from: Moscucci M, Kline-Rogers E, Share D, et al. Simple bedside additive tool for prediction of in-hospital mortality after percutaneous coronary interventions. Circulation 2001;104(3):263-268.)
Figure 4.2 Mayo clinic risk score for major cardiovascular complications of percutaneous coronary intervention (PCI) (in-hospital death, Q-wave myocardial infarction, urgent or emergent coronary artery bypass surgery, and stroke) after coronary intervention assigns integer coefficients for each named clinical variable and reads the estimated mortality risk that corresponds to the total of the integer coefficients from the curve and the valve on the V-axis (Reproduced with permission from: Singh M et al. Correlates of procedural complications and a simple integer risk score for percutaneous coronary intervention. J Am College Cardiol 2002;40(3):387-393).22
Interventional Procedures
Coronary interventions may produce myocardial infarction by a variety of mechanisms that include dissection, abrupt vessel closure, “snowplow” occlusion of side branches, spasm of the epicardial or arteriolar vessels (no reflow), thrombosis, or distal embolization (see Chapters 28 and 29). Q-wave myocardial infarction was reported in 4.8% of patients in the first NHLBI registry and 3.6% in the second NHLBI registry.17 This includes roughly half of the 6% of percutaneous transluminal coronary angioplasty (PTCA) patients who were sent for emergency bypass surgery owing to abrupt vessel closure.16 Over the last decade, experience with coronary stenting has led to marked reduction in the need for emergency bypass surgery (to roughly 0.2%; see Chapters 28 and 31), and accordingly the incidence of Q-wave infarction has fallen to <1%.
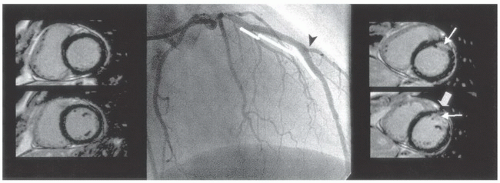
Figure 4.3 Two basal short-axis images (left) in a patient before left anterior descending coronary artery (LAD) percutaneous coronary intervention (PCI) showing no delayed hyperenhancement. Contrast-enhanced images in the same image plane after PCI (right) reveal new anterolateral wall hyperenhancement (long arrows) adjacent to LAD stent (block arrow). Middle panel shows post-PCI angiogram with position of 3 stents highlighted and good flow in LAD and second diagonal branch (likely affected territory; black arrowhead). (Reproduced with permission from: Selvanayagam JB, et al. Circulation 2005;111:1027-1032.)
Largely as a spin-off of trials conducted with the platelet glycoprotein IIb/IIIa receptor blockers in the mid-1990s, however, the official definition of periprocedural myocardial infarction has now been broadened to include non-Q-wave infarctions (more properly called non-ST-elevation myocardial infarctions) detected by elevation of cardiac biomarkers above the 99th percentile of upper limit of normal.26 According to the updated universal definition of myocardial infarction,27 PCI-related myocardial infarction (type 4a) is defined as a cardiac CK-MB or troponin elevation of >3× the upper reference limit in patients with normal baseline levels (see Chapter 28 for a more extensive discussion). Patients with these low-level enzyme elevations are more likely to have some degree of chest discomfort due to occlusion of small side branches or distal microembolization28,29 (Figure 4.3), but this finding is common also in patients without enzyme elevation, where it presumably represents stimulation of adventitial pain receptors by local stretching at the treatment site.30
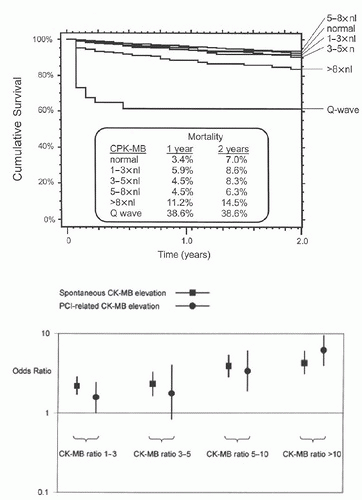
Several studies have evaluated the relationship between elevations of CK-MB and long-term mortality. Although elevation above five or eight times normal corresponds to a significant amount of myocardial necrosis and carries the same adverse impact on long-term prognosis as a Q-wave infarction (Figure 4.4A), long-term follow-up of patients from several multicenter trials32 has shown that patients with even low-level (one to three times normal) elevation of postprocedural CK after PCI have a greater incidence of late adverse outcomes (Figure 4.4B). Similar results have been shown by analysis evaluating the relationship between troponin elevations and long-term mortality.33,34 Whether any such relationship is cause and effect, or simply an association of both periprocedural cardiac biomarker elevation and late events with a common confounding variable (such as the diffuse underlying atherosclerosis) remains to be determined.35,36 However, it has also been suggested that due to the higher sensitivity of troponin, a larger percentage of patients will meet the definition of 4a myocardial infarction when troponin is used when compared to the same patients when CK-MB is used. Some of these patients will not have any evidence of myocardial necrosis even when a very sensitive imaging modality such as contrast-enhanced CMR is used.37
Figure 4.4 Mortality analysis for CK-MB elevation postintervention shows clear effect only for CK-MB greater than five to eight times normal. However, some other analyses suggest that lowerorder CK elevations are also associated with increased mortality. (Top, See reference.31 Bottom, from Akkerhuis KM, et al. Minor myocardial damage and prognosis: are spontaneous and percutaneous coronary intervention —related events different? Circulation 2002;105: 554-556.)
CEREBROVASCULAR COMPLICATIONS
Cerebrovascular accidents (strokes) are uncommon but potentially devastating complications of diagnostic cardiac catheterization. Early experience showed an incidence as high as 0.23% in the 1973 study of Adams and others,38 compared with the 0.07% incidence for the more recent diagnostic catheterizations included in the Society for Cardiac Angiography registries.4,5 Every invasive cardiologist should be familiar with potential etiologies, preventive strategies, and treatments for catheterization-related stroke, and should develop the routine habit of speaking with the patient directly at the end of the procedure. If the patient is less alert, has slurred speech, and either visual, sensory, or motor symptoms during or after a left heart procedure, there should be a low threshold for performing a screening neurologic exam or obtaining an urgent stroke neurology consultation. For major hemispheric events, an urgent carotid angiogram and neurovascular rescue should be considered (usually with a prior computed tomography [CT] or magnetic resonance [MR] scan to exclude hemorrhage), in the hope that neurovascular rescue will minimize the risk of major long-term neurologic deficit or death (if a qualified neurointerventionalist is available).39
The risk of stroke is somewhat higher with coronary intervention, as expected based on the use of guiding catheters, multiple equipment exchanges in the aortic root, aggressive anticoagulation, and longer procedure times. A review of 12,407 patients who underwent PCI at the Washington Hospital Center40 showed a 0.38% risk of per-procedural stroke (roughly half hemorrhagic and half embolic). Risk factors included age older than 80 years, use of an intraaortic balloon pump, and saphenous vein graft intervention. Patients who sustained a stroke had a 37% in-hospital and 56% 1-year mortality, compared with 1.1% in-hospital and 6.5% 1-year mortality in patients who did not sustain a stroke.
Although cerebral hemorrhage must always be excluded, the main cause of catheterization-related strokes seems to be embolic. There is some evidence that many such emboli are dislodged from unsuspected aortic plaque or diffuse atherosclerosis, given the observation that atherosclerotic debris is liberated from the wall of the aorta in 40% to 60% of cases during advancement of large-lumen guiding catheters over a 0.035-inch guidewire.41 Sensitive measures such as transcranial Doppler monitoring of the middle-cerebral artery shows common high-intensity transients during contrast injections or catheter movements,42 and diffusion-weighted magnetic resonance imaging (MRI) before and after retrograde left heart catheterization shows ≤20% incidence of scan defects (but only a 3% neurologic event rate) when aortic stenotic valves are crossed.43 Most neuroophthalmologic complications (i.e., retinal artery embolization)44 and the syndrome of diffuse cholesterol embolization45 also appear to be caused by emboli released by disruption of unrecognized plaques on the walls of the aorta, liberating cholesterol crystals, calcified material, or platelet-fibrin thrombus into the aortic root.
So, we routinely advance our end-hole (i.e., coronary angiographic or, particularly, guiding) catheters around the arch to the ascending aorta over the guidewire, and we pay careful attention to flushing and injection technique, and to minimizing dwell time of guidewires in the aortic root of patients who are not fully anticoagulated (see Chapter 6). There can be no excuse, however, for contributory technical malfeasance such as sloppy catheter flushing, introduction of air bubbles during contrast injection, inadvertent placement of wires and catheters into the arch vessels, prolonged (>3 minutes) wire dwell times during attempts to cross a stenotic aortic valve, or failure to carefully wipe and immerse guidewires in heparinized saline before their reintroduction during left-sided heart catheterization.
In addition to aortic root sources, embolic material may also originate in the cardiac chambers, thrombotic coronary arteries, or the surface of cardiac valves. One should thus avoid placing the pigtail catheter fully out to the left ventricular apex in patients with suspected aneurysm or recent myocardial infarction, since either condition may be associated with potentially dislodgeable mural thrombus. A clot contained in an occluded native coronary artery or vein graft can also be inadvertently withdrawn or propelled out of that vessel and into the aortic root during attempted coronary intervention or forceful injection of contrast through a distal superselective catheter. Care must also be taken to avoid transseptal catheterization or mitral valvuloplasty in patients with left atrial thrombus, which may increase the incidence of clinical stroke. Even avoiding such patients, there is an unexpectedly high incidence of new hyperintense brain lesions by MRI after percutaneous balloon mitral valvuloplasty46 suggesting that small subclinical emboli may occur more commonly than previously suspected. In patients with right-to-left shunting (including atrial septal defects with Eisenmenger physiology and patients with right ventricular infarction and a patent foramen ovale), paradoxic embolization may also lead to stroke. In such patients, the same level of care regarding flushing catheters and sheaths that is routine during left heart procedures should also be extended to right heart procedures.
The question of embolic risk also invariably comes up when it is necessary to perform catheterization on patients with endocarditis of left-sided (aortic and mitral) heart valves. Although these vegetations look friable and can embolize spontaneously, they have already withstood repeated trauma from opening and closing of the affected valves without dislodgment. In a series of 35 patients with active endocarditis who underwent left-sided cardiac catheterization (five of whom had prior spontaneous systemic emboli), none had a catheterization-induced embolic event.47 With current noninvasive techniques for assessing the left ventricle and mitral valve, it is not necessary to enter the left ventricle in a patient with left-sided endocarditis.
Beyond cerebrovascular emboli from intracardiac, arterial, or catheter sources, patients receiving aggressive anticoagulation, antiplatelet, or thrombolytic therapy are also prone to spontaneous intracerebral bleeding as a potential cause for postprocedure neurologic complications. If any doubt exists, and particularly if thrombolytic therapy or intensive anticoagulation is being considered as treatment for a presumptive cerebrovascular embolus, neurologic consultation and CT or MRI scanning are advisable. The distinction is critical, because there have been reported cases of resolution of embolic strokes that occurred during cardiac catheterization after selective infusion of a thrombolytic into the occluded cerebral vessel,39 as well as successful treatment of patients with posterior fossa bleeds as the result of prompt recognition and neurosurgical evacuation.
LOCAL VASCULAR COMPLICATIONS
Local complications at the catheter introduction site are among the most common problems seen after cardiac catheterization procedures, and probably are the single greatest source of procedure-related morbidity. Specific problems include vessel thrombosis, distal embolization, dissection, poorly controlled bleeding at the puncture site, the development of pseudoaneurysm, arteriovenous fistula, retroperitoneal hematoma, and the development of femoral neuropathy. Ongoing bleeding may be owing to a poorly placed puncture, vessel laceration, excessive anticoagulation, or poor technique in either suture closure, mechanical groin compression, or use of a puncture-sealing device (see Chapters 6, 7, and 8).
With the femoral approach, poorly controlled bleeding may present as free hemorrhage, femoral or retroperitoneal hematoma, pseudoaneurysm, or arteriovenous fistula. Although frank hemorrhage and hematoma are generally evident within 12 hours of the procedure, the diagnosis of pseudoaneurysm may not be evident for days or even weeks after the procedure. Given the common and troublesome nature of postprocedural vascular complications, all cardiac catheterization operators must understand vascular access and closure techniques completely to recognize and treat each type of complication. Early experience with the femoral approach by Judkins and others reported a 3.6% local complication rate,48 but the Society for Cardiac Angiography registries reported a 0.5% to 0.6% incidence of vascular complication for diagnostic catheterization, which was similar for the brachial and femoral approaches.7 Brachial complications tend to be thrombotic whereas femoral complications tend to be hemorrhagic, but exceptions to this general rule can and do occur. Complications of radial artery access are described in Chapter 7.
Femoral Artery Thrombosis
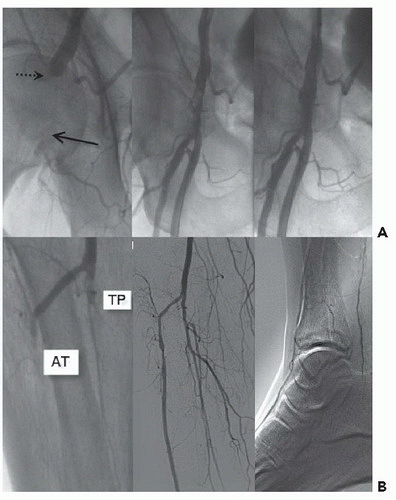
Femoral artery thrombosis can occur in patients with a small common femoral artery lumen (peripheral vascular disease, diabetes, female gender), in whom a large-diameter catheter or sheath (e.g., an intraaortic balloon pump) has been placed, particularly when the catheter dwell time is long or when prolonged postprocedure compression is applied. Such patients have a white painful leg with impaired distal sensory and motor function, as well as absent distal pulses. If this develops during the catheterization procedure and is not corrected promptly by sheath removal, a flow-obstructing dissection or thrombus at the femoral artery puncture site or a distal arterial embolus should be suspected. This requires urgent attention via vascular surgery consultation (for exploration and correction of any local dissection or plaque avulsion and Fogarty embolectomy of the distal vessel as needed to restore distal pulses). Alternatively, operators skilled in peripheral intervention may be able to puncture the contralateral femoral artery, cross over the aortic bifurcation, and address a common femoral occlusion percutaneously49 (Figure 4.5). Either way, failure to restore limb flow within 2 to 6 hours may result in extension of thrombosis into smaller distal branches, with muscle necrosis requiring fasciotomy or even amputation, and predispose to the development of renal failure.
Femoral Vein Thrombosis
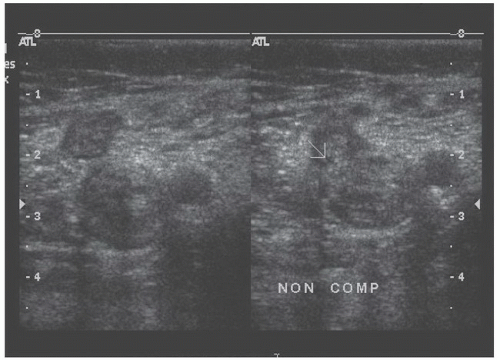
Femoral venous thrombosis and pulmonary embolism are rare complications of diagnostic femoral catheterization (Figure 4.6). A small number of clinical cases have been reported, however, particularly in the setting of venous compression by a large arterial hematoma, sustained mechanical compression (see Chapter 6), or prolonged procedures with multiple venous lines (e.g., electrophysiologic studies).50 However, the actual incidence of thrombotic and pulmonary embolic complications may be substantially under-reported, since most are not evident clinically. Asymptomatic lung scan abnormalities have thus been described in up to 10% of patients after diagnostic catheterization.51
Hemorrhagic Complications
Although thrombotic complications do occur, poorly controlled bleeding from the arterial puncture site is a more common problem after cardiac catheterization by the femoral approach.52 Uncontrollable free bleeding around the sheath suggests laceration of the femoral artery. If such free bleeding does not respond to replacement with the next larger diameter sheath, the bleeding should be controlled by manual compression around the sheath until the procedure is completed. Anticoagulation may be reversed, and an attempt made to remove the sheath and control bleeding with prolonged (30- to 60-minute) compression or to place a femoral closure device (see Chapter 6). The vascular surgeons should be consulted regarding operative repair should the bleeding continue.
Figure 4.5 Femoral artery thrombosis. The morning after AngioSeal closure of the right femoral artery, this patient experienced sharp pain and swelling at the site, managed by 30 minutes of compression. After that, he reported severe pain and loss of sensation in a white limb. Upper left. Crossover from the contralateral side showed occlusion of the common femoral with reconstitution (arrow). Upper center. After balloon dilation, there was a prominent filling defect consistent with thrombus. Upper right. After AngioJet thrombectomy, the filling defect has decreased in size. Lower left. Distal injection, however, showed thrombotic occlusion of both the anterior tibial (AT) and the tibioperoneal (TP) trunk. Lower center. After catheter suction, patency of these vessels was restored. Lower right. Distal angiogram shows filling of both the dorsalis pedis and posterior tibial vessels. (Case courtesy of Dr. Andrew Eisenhauer, Brigham and Women’s Hospital.)
Figure 4.6 Deep venous thrombosis postcatheterization. This 63-year-old man had an 8F AngioSeal device used to close the arterial puncture site in the right groin. When the patient sat up 18 hours after the procedure, he developed acute pain and swelling in the right groin. Manual pressure was held during 20 minutes for suspected groin hematoma. Ultrasound was performed for the presence of a bruit and showed that the femoral vein was not compressible (right panel,arrow), indicating femoral thrombosis. In addition to therapy with aspirin and clopidogrel, anticoagulation was initiated with enoxaparin until adequately anticoagulated with oral warfarin. (Case provided courtesy of Dr. Marie Gerhard-Herman, Brigham and Women’s Hospital.)
Formation of a hematoma—a collection of blood within the soft tissues of the upper thigh—is more common than free bleeding. It tends to cause a tender mass the size of a baseball or softball. If ongoing bleeding stops with manual compression, the hematoma will usually resolve over 1 to 2 weeks as the blood gradually spreads and is reabsorbed from the soft tissues. Larger hematomas may require transfusion, but surgical repair of a hematoma (as opposed to a false aneurysm, see later section) is generally not required. Given the discomfort caused by large hematomas, and the potential of such hematomas to evolve into false aneurysms, accurate puncture and puncture site compression or closure technique to minimize hematoma formation are essential parts of good catheterization technique.
The level of anticoagulation and antiplatelet therapy as well as increased sheath size, female gender, and advanced age all increase the risk of hemorrhagic complications. During the era (1990-1996) when uninterrupted transition from intravenous heparin to oral warfarin was used for stenting, vascular complications were as high as 10%.53 Even before the switch to less aggressive anticoagulant protocols (aspirin and ticlopidine or clopidogrel), second-generation stents that permit use of smaller 6F sheaths, and the widespread use of punctureclosure devices, the incidence of hemorrhagic access site complications after stenting remains at 1% to 2% (see Chapter 6). The tendency of platelet glycoprotein IIb/IIIa blockers to increase local hemorrhagic complications, however, has been tempered by lower levels of heparinization and the growing use of bivalirudin as an alternative antithrombotic agent associated with a lower risk of bleeding.54 Various approaches for collagen plugging or percutaneous suture-mediated closure of the femoral arterial puncture site have been introduced in the last several years (see Chapter 6). Although these devices avoid the discomfort of prolonged manual or mechanical compression and allow earlier or even immediate ambulation, clinical trials have failed to demonstrate significant reduction of major vascular complications compared with those caused by compression.55 It is possible that this class of devices will improve sufficiently to make closure of the femoral artery puncture site so reliable as to eliminate the 1% to 2% incidence of complication. Until that time, operators must be prepared to recognize and repair them when they occur or to work from other access sites such as the radial artery (where hemorrhagic complications are unheard of, and thrombosis [with a negative Allen test] is usually inconsequential) (see Chapter 7), in patients at high risk for a femoral complication.
Only gold members can continue reading. Log In or Register to continue