(1)
Department of General surgery, Fuwai Hospital, Beijing, China
25.1 General Considerations
TGA, also referred to as transposition of the great arteries, is a case in which the primary arteries (the aorta and the pulmonary artery) are transposed rather than being in an abnormal position. TGA is a congenital cardiac malformation characterized by atrioventricular concordance and ventriculoarterial discordance (Fig. 25.2).
In the patient with TGA, the aorta is in front of the pulmonary artery and the plate line of the AV ring is higher than the pulmonary artery. If the aorta is right anterior of the pulmonary artery, the condition is called dextro-transposition TGA (D-TGA); if the aorta is left anterior of the pulmonary artery, it is called levo-transposition TGA (L-TGA). The aorta and the pulmonary artery rise from different ventricles separately, rather than from a common chamber. If the connection of the valves of the arteries and ventricles is normal, the condition is called malposition of the great arteries, in which case, the position of the arteries could be abnormal.
In the case of TGA, the arterial cone suffers dysplasia during the embryonic period, and the mechanism includes abnormal rotation and abnormal absorption of the arterial cone.
In clinic, we can classify patients with TGA by these features:
1.
VSD or not
2.
Pulmonary stenosis
3.
Pulmonary hypertension
4.
Developmental condition of ventricles
5.
Disposition of the atria and ventricle
6.
With other malformations
In the case of TGA, the aorta receives venous blood from the right atria, arterial oxygen saturation is reduced, and the patient turns blue.
The classic TGA belongs to SDD (situs solitus, dextro-loop, D-TGA) type in clinic: the formations of the atria and ventricle are similar to the normal ones, but the ascending aorta rises from the right outlet of the RV, the left and right coronary arteries rise from the anterior part of the root of the aorta, and the major pulmonary artery is pushed to a position left posterior of the aorta (Fig. 25.1). The position of the AV is high and far away from the atrioventricular valve; the position of the PV is low, buried deeply between the MV and the TV. Some fibrous connection exists between the pulmonary and mitral valves. In the RV, the TV and a supraventricular crest can be seen. The AV and TV are separated by muscle of the supraventricular crest. If there is a huge VSD, the PV can be seen through the VSD (Fig. 25.10e). A fibrous connection exists between the pulmonary and mitral valves.
25.2 Specimen Demonstrations
25.2.1 Typical TGA, Without Pulmonary Malformation
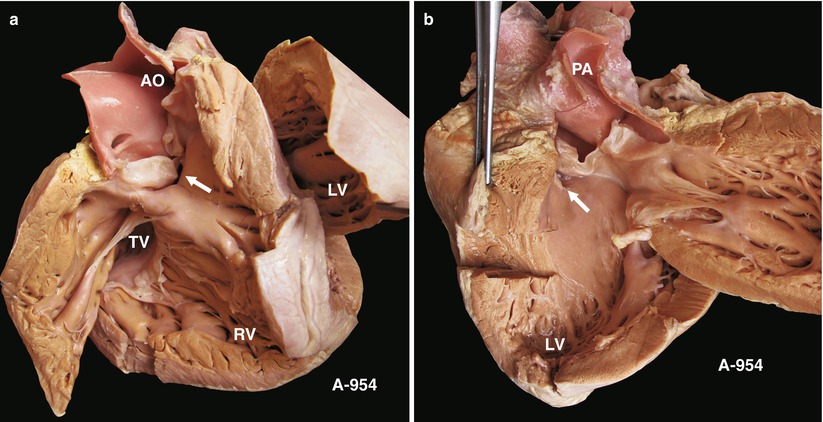
Fig. 25.1
(a) Specimen 954. TGA + VSD aspect of the right ventricle. The aorta rises from the RV. The supraventricular crest is between the aorta and RV. The wall of the RV is very thick. The arrow shows a subarterial VSD. Above all is a classic anatomy case of TGA + VSD. TV tricuspid valve, LV left ventricle, AO ascending aorta. (b) Specimen 954. An aspect of the left ventricle. The pulmonary artery rises from the LV, and a fibrous connection is found between the pulmonary and mitral valves. The arrow shows the VSD under the pulmonary vein. A membranous ventricular septum is anterosuperior of the MV. PA pulmonary artery, LV left ventricle
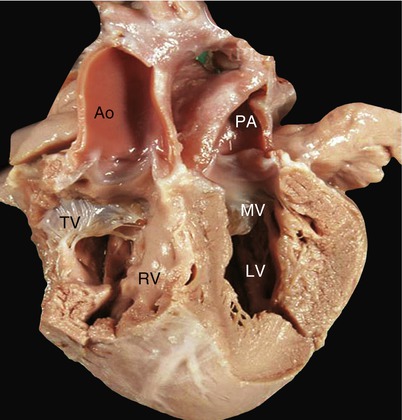
Fig. 25.2
Frontal view of TGA. A long-axis, four-chamber heart aspect shows the anatomical relationship of the TGA: the aorta and pulmonary artery have complete transposition. The supraventricular crest is between the aorta and the TV, and a fibrous connection is between the pulmonary artery and the MV. AO ascending aorta, RV right ventricle, LV left ventricle, PA pulmonary artery
25.2.2 TGA with VSD, Postoperation with RV-PA Bypass
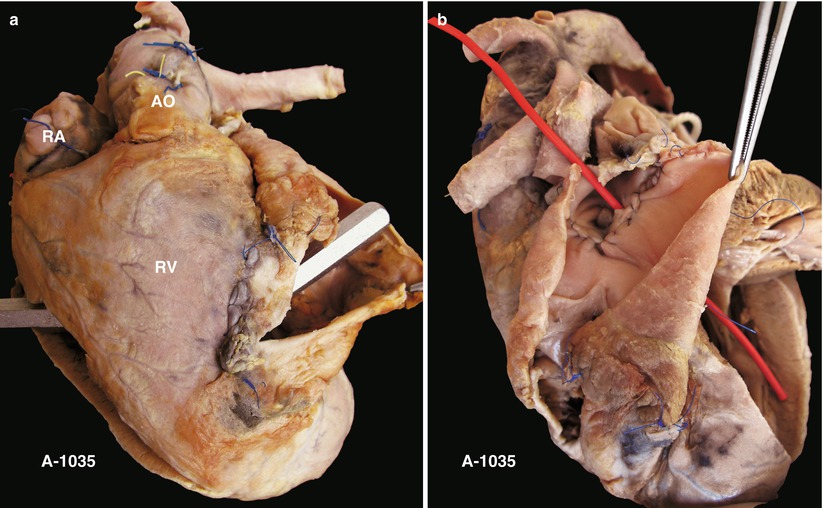
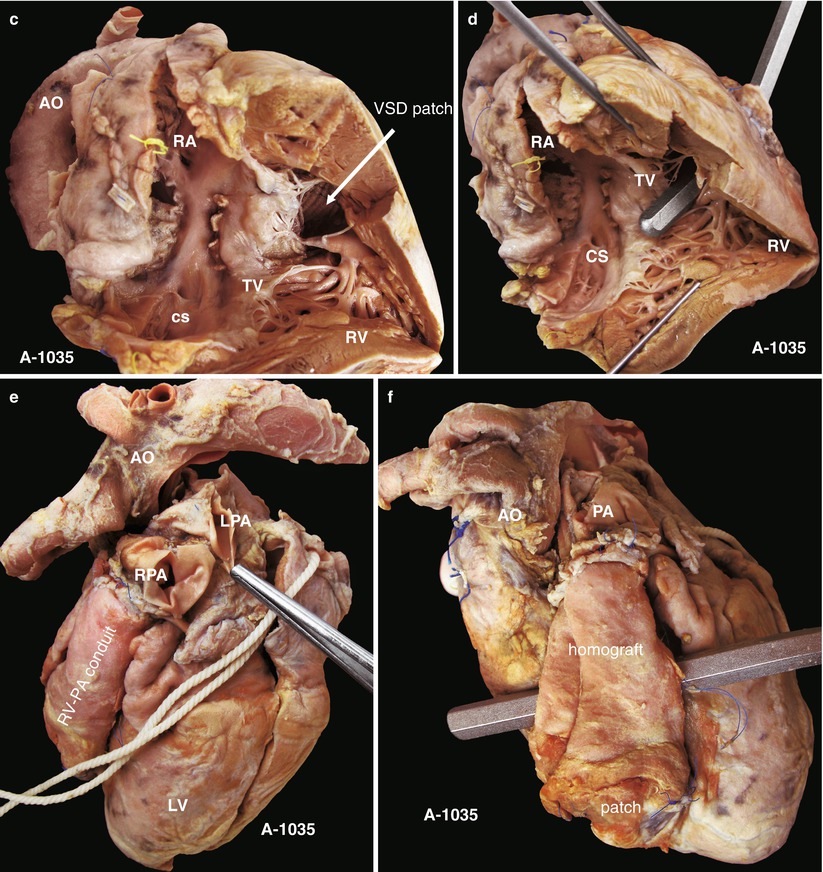
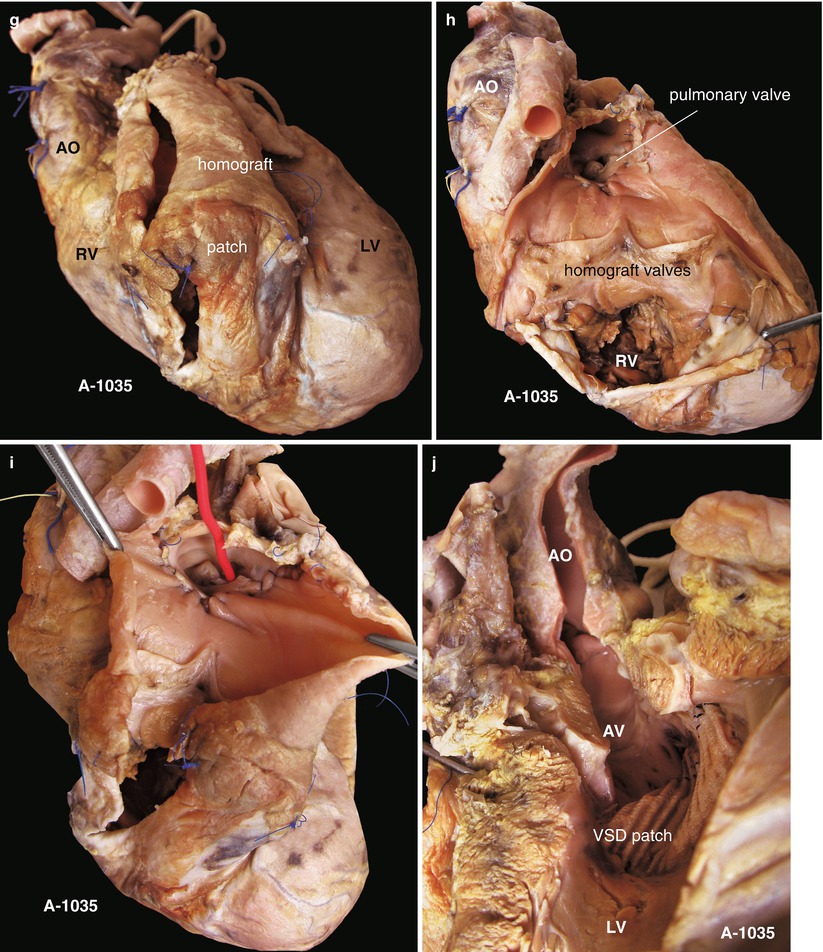
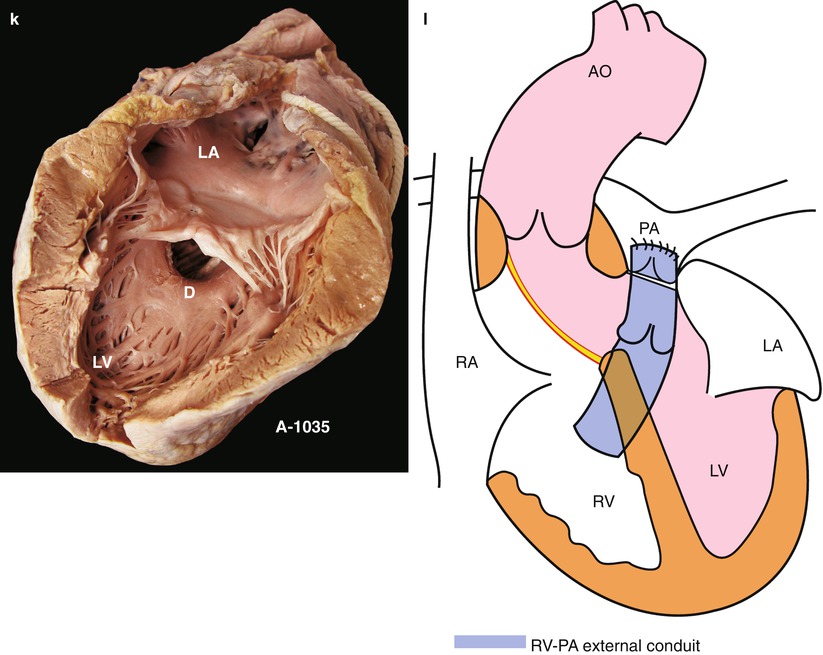
Fig. 25.3
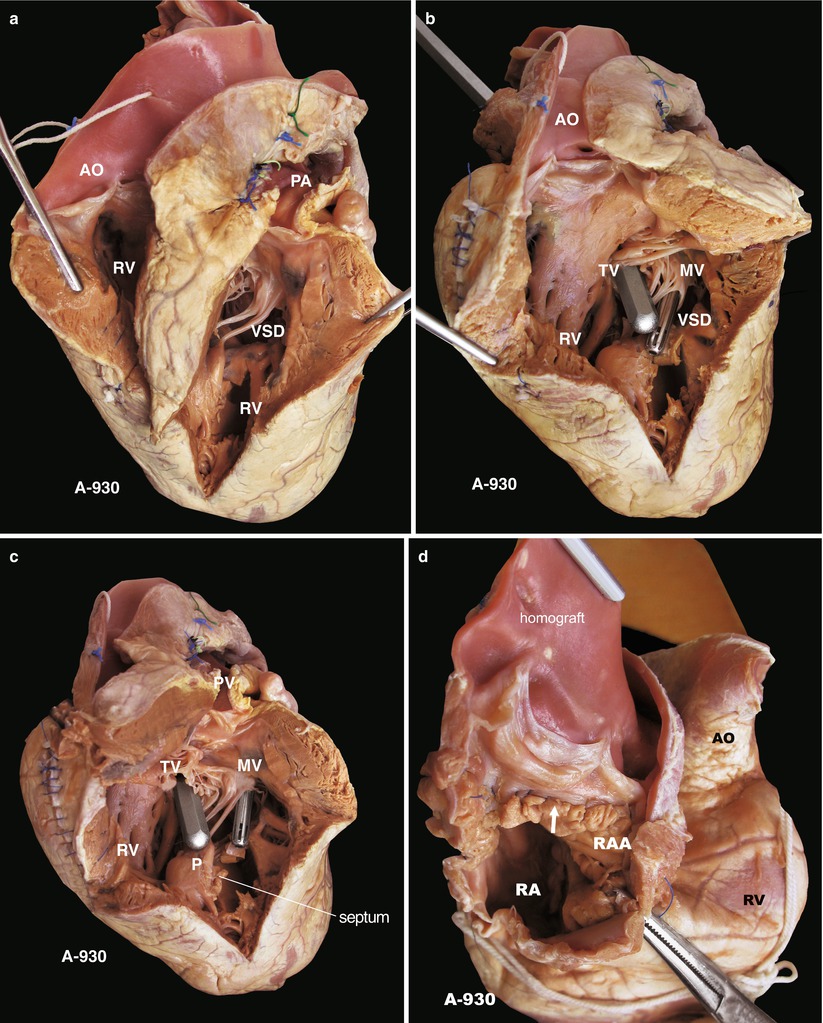
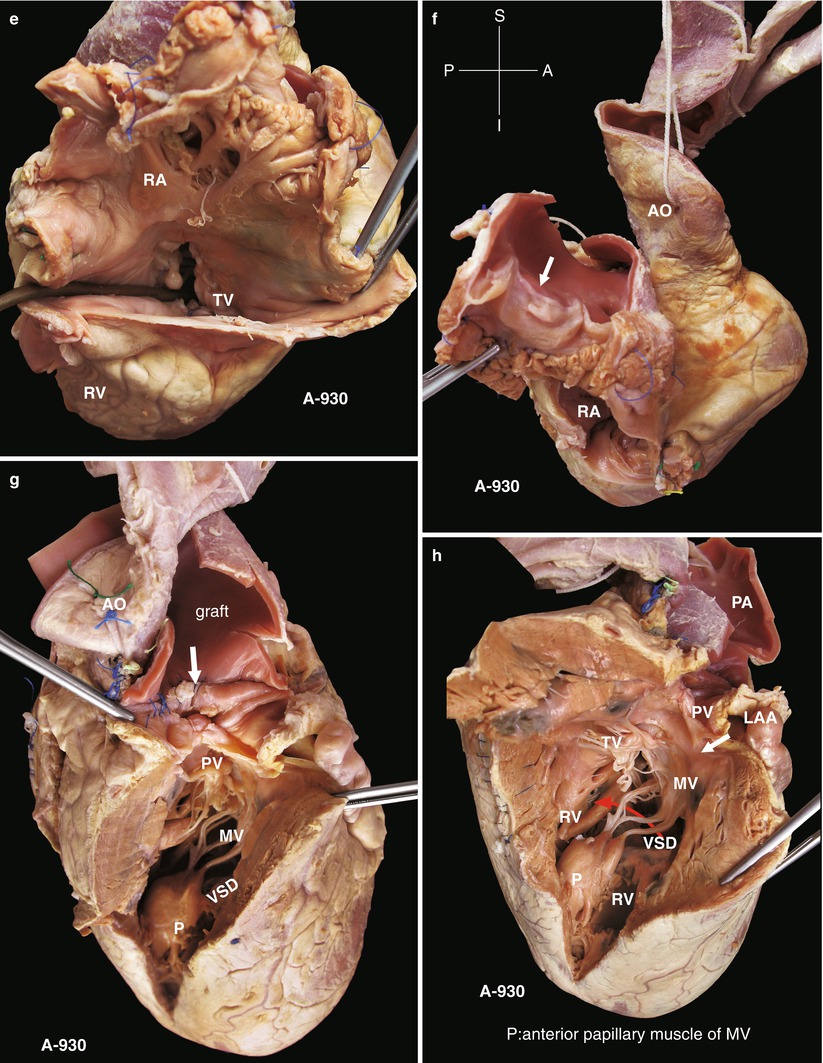
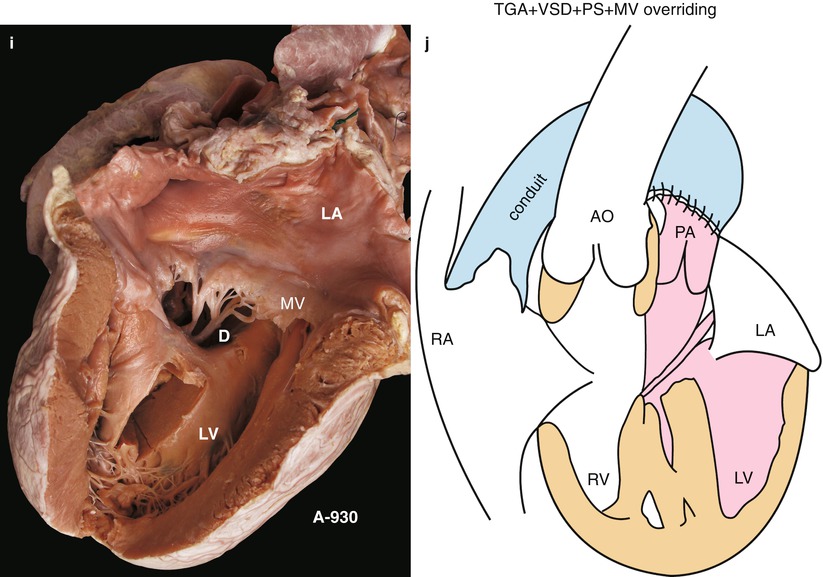
(a) Specimen 1035. Front view of TGA. The aorta rises from the RV; the anatomical position of the atrium and the ventricle is correct, demonstrating a TGA type. The probe is from the RV to the external conduit. RA right atrium, AO ascending aorta. (b) Specimen 1035. Left view of TGA and VSD. The pulmonary artery has a passage to the LV. The red probe is from the PV to the LV, so this case has pulmonary stenosis. An external conduit made of a homograft valved artery is at a junction with the left/right pulmonary artery. (c) Specimen 1035. From right atrium view, the septal leaflet of the tricuspid valve. A revision patch is under the AV and connects the aorta to the LV. Meanwhile, the throughway can be seen from the outlet of the RV to the artificial external conduit. An incision in the front wall of the RV will be selected for the VSD revision and then connected to the external conduit as an entrance. Therefore, a part of the revision patch cannot be seen in this figure. RA right atrium, AO ascending aorta, TV tricuspid valve, RV right ventricle, CS coronary sinus. (d) Specimen 1035. From the right view. The anatomical relationship between the external conduit and RV is shown; the silver probe is inserted into the RV through the external conduit. RA right atrium, TV tricuspid valve, RV right ventricle, CS coronary sinus. (e) Specimen 1035. From the left posterior view. Figure shows the left and right pulmonary arteries, which are well developed, without stenosis. The connection to the external conduit is satisfied. AO ascending aorta, LPA left pulmonary artery, RPA right pulmonary artery, LV left ventricle. (f) Specimen 1035. From left anterior view, showing the unbounded external conduit. The probe crosses through the gap posterior to the external conduit, which means that the conduit is entirely outside the RV, the remote of the external conduit anastomoses to the pulmonary bifurcation. “Homograft” is a homograft valved artery. AO ascending aorta, PA pulmonary artery. (g) Specimen 1035. From front view. Figure shows the external conduit from the RV to the pulmonary artery. The upper part of the conduit is an artificial patch, and the lower part is a homograft valved artery. The left anterior descending artery is next to the conduit. AO ascending aorta, RV right ventricle, LV left ventricle. (h) Specimen 1035. From cutaway view of the external conduit. Figure shows the homograft valves; the opening of the PV is closed, and the external conduit is directly connected to the pulmonary artery. The blood in the RV flows into the pulmonary artery through the external conduit, and the blood in the LV flows into the aorta. “RV” indicates the anastomosis between the RV and the external conduit. AO ascending aorta. (i) Specimen 1035. From left upper view. Figure shows the relationship of the pulmonary artery opening and the RV. The red probe is inserted into the LV through a gap of the pulmonary artery, which excludes the diagnosis of DORV. (j) Specimen 1035. Cutaway into the aorta and left ventricle. The valves of the aorta rise from the RV, and a VSD patch blocks the aorta to the LV, which becomes a part of the LV outlet. The patch also can be thought of as an inner channel of isolated blood flow from the LV to the aorta. AO ascending aorta, AV aortic valve. (k) Specimen 1035. From left lateral view, the structure of the left atrium and ventricle. A defect (D) is on the top of the ventricular septum, and the MV has a little cleft in the anterior leaflet, the border of which is fibrous and thick. LA left atrium, LV left ventricle. (l) Specimen 1035. Spatial structure diagram of postoperation. A VSD patch connects the aorta to the LV, and an external conduit connects the pulmonary artery to the RV; the pulmonary valve opening is closed. AO ascending aorta, PA pulmonary artery, LA left atrium, RA right atrium
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


