The aim of this study was to assess whether coronary computed tomographic angiography (CCTA) would allow accurate length measurements that may help select optimal stent length. In 19 patients who underwent stent implantation and CCTA, the lengths of 30 implanted stents were assessed independently using quantitative coronary angiography (QCA) at the time of implantation and CCTA during follow-up. Measurements on CCTA and QCA were compared with the actual lengths of the implanted stents. The mean actual stent length was 17.3 ± 6.3 mm; the mean length of the stents measured using CCTA was 17.25 ± 5.54 mm, and the mean length of the stents measured using QCA was 15.92 ± 5.86 mm. There was a stronger positive correlation between measurements on CCTA versus actual stent lengths (R = 0.99, p = 0.0001) than between measurements on QCA versus actual stent lengths (R = 0.82, p = 0.0001) (p <0.0001 for the difference between correlation coefficients). In conclusion, the length measurements obtained with CCTA correlate better with an anatomic gold standard (actual stent lengths) than those obtained using QCA.
Coronary computed tomography angiography (CCTA), a noninvasive method of imaging the coronary arteries, is a valuable diagnostic procedure for selected patients. Although CCTA is complementary to quantitative coronary angiography (QCA) in the estimation of coronary tree dimensions, the accuracy of the information provided by CCTA may differ from that of the information provided by QCA. The length of a lesion, and consequently the optimal length of the stent, is decided routinely either on the basis of the operator’s visual estimation or findings on QCA, with infrequent guidance by intravascular ultrasound. The purpose of this retrospective study was to compare the accuracy of length measurements on CCTA and QCA using known stent lengths as an anatomic reference.
Methods
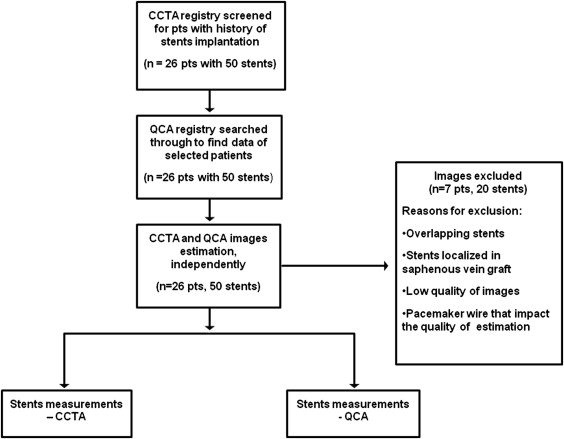
The Warsaw Institute of Cardiology prospective coronary computed tomographic (CT) angiographic diagnostic procedure registry was searched to identify patients studied from May 2008 to September 2010 with histories of coronary artery stent implantation and follow-up CCTA within 24 months. The exclusion criteria were (1) overlapping stents, (2) saphenous vein graft location of the implanted stent, and (3) poor quality of the diagnostic images. A study overview is shown in Figure 1 .
The actual stent length was retrieved from the procedure log. It was assumed that the length of the stent obtained from the device label would be an absolute marker of distance and that stent length remained constant during follow-up.
Coronary CT angiographic data were acquired using a dual-source CT scanner (Somatom Definition; Siemens Medical Systems, Forchheim, Germany). All coronary CT angiographic studies were performed after sublingual administration of nitrates (0.8 mg), and patients with heart rates >65 beats/min additionally received β-blocking medication (metoprolol 2.5 to 10 mg) intravenously. An electrocardiographically gated retrospective acquisition protocol was used in all patients, with 330-ms rotation time, 0.6-mm collimation, and 80- to 140-kV tube voltage adjusted manually for body mass index. Dual-source CT images were stored on digital media for off-line analysis. Off-line dual-source CT data were analyzed using quantitative coronary CT angiographic software (Circulation; Siemens Medical Systems). All measurements were made manually on cross-sectional arterial reconstructions by a reader blinded to the measurements on QCA. The stent length was measured as the distance between the first and last visualized strut of the stent. An average of 3 measurements was taken as the final coronary CT angiographic length.
Coronary angiograms were acquired using a Siemens angiograph (AXIOM Artus DFC; Siemens Medical Systems). Data from visual estimation and QCA were recorded and used for analyses. QCA was performed using a computer-assisted quantitative coronary arteriographic edge detection algorithm (ACOMPC; Siemens Medical Systems); a contrast-filled catheter was used for calibration. All angiograms were analyzed independently by experienced observers blinded to the measurements on CCTA. The best projection obtained at the time of stent implantation was chosen. The assumption was made that the projection showing stent expansion was the best projection to minimize foreshortening. Stent length was measured from the first to the last visualized strut of the stent. An average of 3 measurements was taken as the final quantitative coronary angiographic length.
All statistical analyses were performed using MedCalc version 9.3.8.0 (MedCalc Software, Marierkerke, Belgium). Continuous data with normal distribution are presented as mean ± SD. Two-tailed paired-sample Student’s t tests were used to assess differences between continuous variables. Linear regression was used to compare actual stent length with the measurements obtained with QCA and CCTA. Fisher’s r-to-z transformation was used to compare the difference between 2 correlation coefficients. Bland-Altman plots were produced to visualize the difference between measurements by the different imaging techniques, and a 2-tailed paired-sample Student’s t test was used to compare that difference.
Results
Fifty stents from a population of 26 patients were identified and measured. We excluded patients with overlapping stents (n = 9), stents located in saphenous vein grafts (n = 8), images of low quality caused by calcification (n = 2), and pacemaker wires in the right ventricle obscuring the right coronary artery (n = 1). As a result, a total of 30 stents in 19 patients were measured with CCTA and QCA. Basic demographic and clinical characteristics of patients are listed in Table 1 .
| Patient | Age (yrs)/Gender | Stented Artery No. 1 | Stented Artery No. 2 | Stented Artery No. 3 | Interval Between QCA and CCTA (mos) | Previous Myocardial Infarction | Diabetes Mellitus | Obesity (BMI >30 kg/m 2 ) | Hypertension | Hypercholesterolemia | Active Smoker | Arrhythmias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 49/M | LCx | — | — | 10 | 0 | 0 | + | 0 | + | 0 | 0 |
| 2 | 50/M | RCA | — | — | 20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 | 55/F | LAD | — | — | 13 | 0 | 0 | 0 | 0 | 0 | + | + |
| 4 | 56/M | LAD | — | — | 7 | 0 | 0 | 0 | + | 0 | 0 | 0 |
| 5 | 56/M | LAD | RCA | RCA | 8 | + | + | + | + | + | + | 0 |
| 6 | 57/M | RCA | RCA | — | 13 | 0 | 0 | + | + | + | + | 0 |
| 7 | 58/M | LAD | RCA | — | 18 | 0 | 0 | 0 | 0 | + | + | 0 |
| 8 | 59/F | LAD | — | — | 7 | 0 | 0 | + | 0 | + | + | 0 |
| 9 | 63/M | LCx | RCA | — | 24 | 0 | 0 | 0 | + | 0 | + | 0 |
| 10 | 63/M | RCA | RCA | RCA | 6 | + | + | + | + | + | 0 | 0 |
| 11 | 65/F | LAD | — | — | 21 | + | + | + | + | + | 0 | 0 |
| 12 | 69/F | RCA | — | — | 10 | 0 | 0 | + | + | + | 0 | + |
| 13 | 76/M | LCx | — | — | 13 | + | 0 | 0 | + | + | + | + |
| 14 | 76/F | LAD | LAD | — | 7 | + | + | + | + | + | 0 | 0 |
| 15 | 76/M | LAD | RCA | — | 6 | + | + | + | + | + | + | 0 |
| 16 | 77/M | LCx | — | — | 16 | + | 0 | + | + | + | 0 | 0 |
| 17 | 77/F | LAD | — | — | 24 | 0 | 0 | 0 | + | + | 0 | + |
| 18 | 79/M | RCA | RCA | — | 15 | + | 0 | 0 | + | + | + | + |
| 19 | 84/M | RCA | RCA | — | 6 | + | 0 | 0 | + | + | + | + |
The mean actual stent length was 17.3 ± 6.3 mm; mean stent lengths measured using CCTA and QCA were 17.3 ± 5.5 and 15.92 ± 5.86 mm, respectively. The difference between measurements on CCTA and actual stent lengths was not significant (p = 0.80), but the stent lengths measured by QCA were significantly shorter than the actual stent lengths (p = 0.02). There was a stronger positive correlation between stent length on CCTA and actual stent length (R = 0.99, p = 0.0001) than between stent length on QCA and actual stent length (R = 0.82, p = 0.0001). The difference between correlation coefficients was significant (z = −8.26, p <0.0001). The comparison of 2 regression lines and equations are presented in Figure 2 .



