The aim of this prospective, open-label, cohort study was to compare the effect of muscle functional electrical stimulation (FES) on endothelial function to that of conventional bicycle training. Eligible patients were those with New York Heart Association class II or III heart failure symptoms and ejection fractions ≤0.35. Two physical conditioning programs were delivered: FES of the muscles of the lower limbs and bicycle training, each lasting for 6 weeks, with a 6-week washout period between them. Brachial artery flow-mediated dilation (FMD) and other parameters were assessed before and after FES and the bicycle training program. FES resulted in a significant improvement in FMD, which increased from 5.9 ± 0.5% to 7.7 ± 0.5% (95% confidence interval for the difference 1.5% to 2.3%, p <0.001). Bicycle training also resulted in a substantial improvement of endothelial function. FMD increased from 6.2 ± 0.4% to 9.2 ± 0.4% (95% confidence interval for the difference 2.5% to 3.5%, p <0.001). FES was associated with a 41% relative increase in FMD, compared to 57% with bicycle exercise (95% confidence interval for the difference between the relative changes 1.2% to 30.5%, p = 0.034). This resulted in attaining a significantly higher FMD value after bicycle training compared to FES (9.2 ± 0.4% vs 7.7 ± 0.5%, p <0.001). In conclusion, the effect of muscle FES in patients with heart failure on endothelial function, although not equivalent to that of conventional exercise, is substantial. Muscle FES protocols may prove very useful in the treatment of patients with heart failure who cannot or will not adhere to conventional exercise programs.
In the constellation of pathophysiologic interactions leading to the clinical manifestations of heart failure, endothelial function has emerged as a major player, being at the center of several regulatory mechanisms that become impaired in the process of heart failure progress. Physical exercise has been shown to improve endothelial function in patients with heart failure, although capability to perform or adhere to physical conditioning programs may be a problem. Functional electrical stimulation (FES), a modality that causes muscular contraction through electrical stimulation, could also have a similar beneficial effect, as demonstrated in preliminary studies. The aim of the present study was to compare the effect of lower limb muscle FES on endothelial function, as assessed by the flow-mediated dilation (FMD) of the brachial artery, to that of a conventional physical exercise training program (bicycle training).
Methods
Eligible patients were those with heart failure symptoms New York Heart Association (NYHA) class II or III, of ischemic or nonischemic origin, with ejection fractions ≤0.35. All patients were clinically stable (no admission for heart failure within the previous 6 months, no dyspnea at rest, no lung rales) and received optimized treatment, including β blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, aldosterone antagonists, and furosemide as needed, for ≥2 months before inclusion. No patient followed any physical conditioning program. Patients failing to attend ≥90% of the scheduled training sessions were excluded. All patients provided informed consent, and the study protocol was approved by the competent institutional review boards of Athens General Hospital “G. Gennimatas” and the University of Athens Medical School.
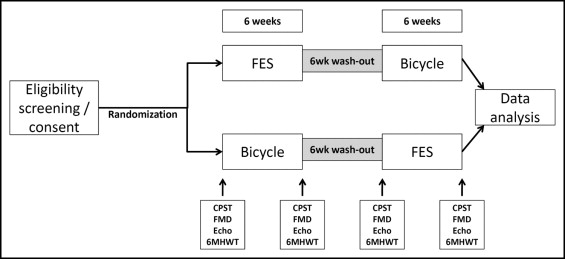
This was a prospective, open, single-group, crossover, cohort study. The studied interventions were 2 different physical conditioning programs: FES of the muscles of the lower limbs and bicycle training, according to predefined protocols, each lasting for a period of 6 weeks, with a 6-week washout period between them (the 6-week duration of training and washout intervals was based on previous observations regarding the exercise effect on endothelium and its persistence after cessation of exercise ). All patients were submitted to the 2 interventions sequentially, after being randomized as to the sequence of the programs ( Figure 1 ). Each patient was assessed at 4 time points ( Figure 1 ): before and after the FES program and before and after the bicycle training program. The primary end point of the study was the FMD differences observed over the time periods of the physical conditioning programs.
Transcutaneous periodic neuromuscular electrical stimulation was applied on the quadriceps and calf (gastrocnemius) muscles of the 2 lower extremities, for 30 minutes daily, 5 days a week, for a period of 6 weeks. The electrodes were placed 5 cm distal to the inguinal ligament and 3 cm proximal to the patella for the quadriceps muscle stimulation, and 3 cm distal to the popliteal fossa and 3 cm proximal to the Achilles tendon insertion for the gastrocnemius muscle stimulation. The intensity of stimulation was adjusted to a level resulting in visible muscle contraction, without causing discomfort for the patient. The stimulator discharges at a frequency of 25 Hz for 5 seconds, followed by a 5-second rest. Treatment sessions were performed in the hospital, under the supervision of a trained physical therapist.
The bicycle training program consisted of 30-minute sessions, using an ergometric bicycle, 5 days a week, for a period of 6 weeks. Exercise intensity was adjusted to achieve 70% of maximal age-predicted heart rate. Exercise was supervised by a trained physical therapist or a research cardiologist.
FMD measurements were made on the right brachial artery. A mark was drawn approximately 2 to 3 cm above the antecubital fossa and was used for ultrasound measurements. Baseline brachial artery diameter and flow were recorded, and subsequently, a blood pressure cuff was inflated at the brachium to 20 mm Hg greater than systolic arterial pressure for 5 minutes. After cuff release, interrogation of brachial artery flow was repeated to demonstrate hyperemia, and the brachial artery diameter was remeasured within 3 minutes after cuff deflation (the artery was scanned continuously over this time period to be able to measure maximal diameter). Images were acquired using a broadband linear array transducer, with a frequency range of 3 to 12 MHz. All measurements were made in a stable-temperature, semidark room, 1 hour after administering oral bromazepam 3 mg. FMD was expressed as percent change in brachial artery diameter after cuff deflation, compared to the preinflation measurement. Endothelium-independent dilation of the brachial artery was measured in a similar manner, substituting the inflation and deflation of the manometer cuff (hyperemia) for sublingual administration of nitroglycerin (400 μg).
The cardiopulmonary stress test was performed with a modified Bruce protocol using standard treadmill gas exchange measurement equipment. Maximal oxygen consumption was calculated and used as a functional status parameter. Transthoracic echocardiography was performed using an iE33 (Philips Medical Systems, Andover, Massachusetts) ultrasound machine. The left ventricular ejection fraction was computed by application of the modified Simpson’s method in the apical 4-, 3-, and 2-chamber views.
Continuous variables (including FMD and endothelium-independent dilation, which are expressed as percentages but represent continuous variables) were compared using Student’s t test for paired data and are expressed as mean ± SEM. Adequate fit of the distribution of studied parameters to the normal distribution was tested with the Kolmogorov-Smirnov test. In case of significant deviation from the normal distribution, nonparametric methods were applied. Categorical variables were compared using chi-square tests or Fisher’s exact test, if the produced matrices contained cells with expected counts <5, and are expressed as counts and percentages. PASW Statistics version 18 was used for statistical analysis (SPSS, Inc., Chicago, Illinois), and p values <0.05 were considered statistically significant.
Results
From 33 initially screened eligible patients, 31 completed the 18-week FES and bicycle training period (24 men, mean age 60.7 ± 2.1 years, range 33 to 79). One patient dropped out because of worsening heart failure, and 1 failed to present for >10% of sessions. Among the rest, no severe adverse events were recorded, and no patient was admitted for heart failure during this period. Twenty-one patients (67.7%) had NYHA class II symptoms, and the remainder (32.3%) had NYHA class III symptoms (mean NYHA class 2.3 ± 0.1). Five patients (16.1%) had histories of chronic obstructive pulmonary disease.
FES was found to be associated with a significant increase in both important functional parameters, leading to a mean increase of 42.9 m in 6-minute walking distance (448.1 ± 17.6 to 491.0 ± 18.4 m, 95% confidence interval [CI] for the difference 35.6 to 50.2, p <0.001) and of 1.1 ml/kg/min in maximal oxygen consumption (17.7 ± 0.9 to 18.8 ± 1.0 ml/kg/min, 95% CI for the difference 0.3 to 1.8, p = 0.006). In comparison, the bicycle exercise program also resulted in substantial amelioration of the studied indexes of functional status. Namely, over the 6-week period of bicycle training, the distance walked in 6 minutes by the patients increased from 446.8 ± 15.6 to 505.0 ± 15.6 m (mean increase 58.2 m, 95% CI 49.5 to 66.9, p <0.001), and maximal oxygen consumption during cardiopulmonary stress testing increased from 18.2 ± 0.9 to 20.8 ± 1.1 ml/kg/min (mean increase 2.6 ml/kg/min, 95% CI 1.6 to 3.6, p <0.001).
Comparison of the differences effected by the 2 modalities on heart failure functional status showed that both conferred a significant benefit, although its extent was larger with bicycle training. This becomes more obvious by comparing the percentage differences associated with the 2 physical conditioning programs ( Figure 2 ). The increases conferred by bicycle training compared to FES on maximal oxygen consumption (14.3% vs 7.4%) and 6-minute walking distance (14.1% vs 10.1%), although comparable and within a similar value range (see box plots in Figure 2 ), differed to a statistically significant extent (p <0.001 for both).



