ST-segment depression during stress testing predicts future risk for adverse cardiovascular events and routinely prompts further noninvasive imaging or invasive evaluation for coronary artery disease (CAD). A subset of patients develop ST depression at peak exercise that rapidly resolves early in the recovery period (ST-rapid). The goal of this study was to compare the prevalence of single-photon emission computed tomographic myocardial perfusion imaging (MPI) findings in patients with ST-rapid to those with prolonged ST depression (ST-prolonged) and those without ST depression (ST-normal). A total of 637 men without previous CAD and with interpretable rest electrocardiograms referred for exercise stress MPI were included in this study. ST depression was defined as ≥1-mm ST depression occurring 80 ms after the J point at peak exercise. ST-rapid was defined as ST depression with recovery of the ST depression by 1 minute into recovery. Men with ST-rapid were younger (55.4 ± 7.6 vs 62.6 ± 9.6 years, p <0.001) and had better exercise capacity (11.2 ± 2.8 vs 9.4 ± 3.0 METs, p <0.001) than men with ST-prolonged. Compared to ST-prolonged, ST-rapid was associated with significantly less mild CAD (summed stress score ≥4; 27% vs 47%, p = 0.02), severe CAD (summed stress score >8; 9% vs 29%, p = 0.004), and a composite of high-risk MPI findings (summed stress score >8 or ejection fraction <40%; 11% vs 32%, p = 0.003). There were no significant differences in exercise capacity, the presence of CAD, or the composite of high-risk MPI findings between men with ST-rapid and those with ST-normal. In conclusion, men who developed ST-rapid during exercise stress testing had markedly fewer abnormal and high-risk MPI findings compared to those with prolonged ST depression. In fact, the prevalence of MPI abnormalities in men with ST-rapid was similar to that in men with normal electrocardiographic responses to exercise.
ST-segment depression occurring during exercise stress testing predicts future risk for adverse cardiovascular events and routinely prompts further noninvasive imaging or invasive evaluation for coronary artery disease (CAD). A subset of patients develop ST-segment depression at peak exercise that rapidly resolves, frequently <1 minute into the recovery period. It is unclear whether such ST-segment depression with rapid recovery (ST-rapid) should be considered a high-risk marker of underlying CAD. Stress single-photon emission computed tomographic myocardial perfusion imaging (MPI) is a widely used noninvasive imaging modality that allows the identification of patients with existing CAD and stratifies cardiovascular prognosis. Thus, the goal of this study was to compare the prevalence of high-risk stress MPI findings in patients with ST-rapid to those in patients with prolonged ST-segment depression (ST-prolonged) and those without ST-segment depression (ST-normal), in men who underwent exercise MPI.
Methods
Eligible subjects were identified from a prospectively obtained database of men referred for exercise stress MPI testing. Men without previous CAD (defined as a history of myocardial infarction or previous coronary revascularization), who were in sinus rhythm with electrocardiograms interpretable for ischemic changes (no ST-segment abnormalities at rest, left branch bundle block, or digoxin therapy), were eligible for inclusion. Men who did not achieve 85% of predicted maximal heart rate were excluded. Cardiovascular risk factors and co-morbidities were recorded. The study protocol was approved by the hospital’s institutional review board, and all patients gave informed consent.
ST-segment depression was defined as ≥1-mm ST-segment depression occurring 80 ms after the J point at peak exercise consistent with previous studies and current practice guidelines. ST-segment depression with rapid recovery (ST-rapid) was defined as ST-segment depression with recovery of the ST-segment depression occurring by 1 minute into the recovery period. ST-prolonged was defined as ST-segment depression that persisted >1 minute into recovery. ST-normal was defined as the absence of ST-segment depression during exercise or in recovery.
Exercise testing consisted of symptom-limited exercise treadmill testing using a Bruce protocol, with a standard 1-minute cool-down (treadmill speed 1 mph, 0% incline). Beta blockers and calcium channel blockers were discontinued 24 to 48 hours before exercise when feasible. All standard exercise testing parameters were recorded. Standard single-isotope (technetium-99m tetrofosmin) or dual-isotope (thallium-201 chloride and technetium-99m tetrofosmin) MPI testing at rest and during stress was performed on all patients. Single-photon emission computed tomographic images were acquired using a dual-headed gamma camera equipped with a high-resolution parallel-hole collimator (ElGems CardiaL, GE Medical Systems, Waukesha, Wisconsin; or Forte, Philips Medical Systems, Cleveland, Ohio). Scans at rest were obtained 10 to 30 minutes after the intravenous injection of 3.0 to 4.5 mCi of thallium-201 chloride for dual-isotope testing or 8 to 15 mCi of technetium-99m tetrofosmin for single-isotope testing. Scans during stress were obtained 15 to 60 minutes after peak stress injection of 24 to 45 mCi of technetium-99m tetrofosmin. The left ventricular (LV) ejection fraction at rest was determined from electrocardiographic (ECG) gating of the poststress technetium-99m myocardial perfusion images.
MPI interpretation was performed at the time of clinical study by 1 of 5 experienced readers, using the 17-segment model approved by the American Society of Nuclear Cardiology. Summed stress scores (SSS), summed rest scores, and summed difference scores were determined for all patients. Mild or greater coronary disease was defined as an SSS ≥4, mild coronary disease only was defined as an SSS of 4 to 8, and severe coronary disease was defined as an SSS >8. LV dysfunction and marked LV dysfunction were defined as ejection fractions <50% and <40%, respectively. The end points of SSS ≥4 and an LV ejection fraction <50% included those with SSS >8 and LV ejection fractions <40%, respectively. A composite end point of any high-risk finding (SSS >8 or LV ejection fraction <40%) was also recorded.
Baseline characteristics and findings on MPI testing for patients with ST-rapid were compared to those of patients with ST-prolonged and ST-normal, respectively, using the chi-square test for categorical variables and Student’s t test for continuous variables, with a 2-tailed p value <0.05 indicating statistical significance.
Results
Overall, 637 subjects met the inclusion criteria and were enrolled in the study. Among this cohort, 80% (n = 509) had no significant ST depression (ST-normal), whereas 20% (n = 128) experienced ST depression. Among those with ST depression, 48% (n = 62) met the criteria for ST-prolonged, and 52% (n = 66) met the criteria for ST-rapid.
Baseline characteristics for all patients in the study stratified by exercise ECG response are listed in Table 1 . Compared to those subjects with ST-prolonged, those with ST-rapid were younger and were less likely to be taking β blockers. Compared to the ST-normal group, those with ST-rapid were of similar age and had no differences in CAD risk factors or medications.
| Variable | ST-Normal (n = 509) | ST-Rapid (n = 66) | ST-Prolonged (n = 62) | p Value ⁎ |
|---|---|---|---|---|
| Age (years) | 56.4 ± 11.6 | 55.4 ± 7.6 | 62.6 ± 9.6 | <0.001 |
| Diabetes mellitus | 21% (107) | 23% (15) | 27% (17) | NS |
| Hypertension † | 53% (270) | 56% (37) | 65% (40) | NS |
| Hyperlipidemia † | 44% (224) | 45% (30) | 48% (30) | NS |
| Tobacco use (current) | 20% (102) | 17% (11) | 26% (16) | NS |
| Medications | ||||
| β blockers | 20% (102) | 18% (12) | 36% (22) | 0.03 |
| Calcium channel blockers | 15% (76) | 15% (10) | 21% (13) | NS |
⁎ Comparison between ST-rapid and ST-prolonged. All comparisons between ST-rapid and ST-normal were not significant.
† Defined as present if documented in the patient’s medical record and the patient was taking medications specifically for the condition.
Exercise stress findings stratified by exercise ECG response are listed in Table 2 . Compared to men with ST-prolonged, those with ST-rapid achieved higher peak heart rates, had better exercise capacity, and were less likely to develop chest pain during exercise. In contrast, compared to those with ST-normal, men with ST-rapid achieved higher percentage predicted heart rates and higher peak pressure products.
| Variable | ST-Normal | ST-Rapid | ST-Prolonged | p Value ⁎ |
|---|---|---|---|---|
| (n = 509) | (n = 66) | (n = 62) | ||
| Rest heart rate (beats/min) | 66.6 ± 12.2 | 65.2 ± 10.8 | 66.5 ± 11.8 | NS |
| Peak heart rate (beats/min) | 159.9 ± 14.3 | 161.2 ± 13.0 | 152.8 ± 14.0 | 0.001 |
| % Predicted heart rate | 97.8 ± 7.5 | 100.1 ± 10.8 † | 96.4 ± 9 | <0.001 |
| Peak pressure product | 28.2 ± 4.5 | 30.0 ± 3.9 ‡ | 26.2 ± 4.5 | <0.001 |
| Exercise time (minutes) | 9.3 ± 3.0 | 9.9 ± 2.5 | 7.9 ± 2.9 | <0.001 |
| METs | 10.8 ± 3.2 | 11.2 ± 2.8 | 9.4 ± 3.0 | <0.001 |
| ST depression (mm) | — | 2.0 ± 0.6 | 2.4 ± 1.0 | 0.01 |
| Duke treadmill score | 8.9 ± 3.6 | −0.8 ± 4.9 ‡ | −6.4 ± 6.7 | <0.001 |
| Duke angina (1 or 2) | 8% (41) | 15% (10) | 40% (25) | 0.003 |
⁎ Comparison between ST-rapid and ST-prolonged.
‡ p <0.01 versus ST-normal. All other comparisons between ST-rapid and ST-normal were not significant.
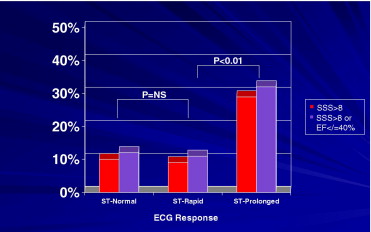
MPI findings for all patients in the study stratified by exercise ECG response are shown in Figure 1 and listed in Table 3 . Compared to men with ST-prolonged, those with ST-rapid had a lower prevalence of mild or greater CAD, severe CAD, and the composite of any high-risk MPI finding but no difference in mild CAD only. In contrast, there were no significant differences in the prevalence of CAD or composite high-risk MPI findings in those with ST-rapid compared to those with ST-normal.