Firefighters are known to have an elevated rate of sudden cardiac death compared to the general population. It is unclear whether this finding is related to underlying cardiovascular risk factors or whether firefighting inherently carries additional risk. Our objective was to determine whether Los Angeles county firefighters have higher coronary artery calcium (CAC) scores and increased atherosclerosis as determined using 64-slice cardiac, multidetector computed tomography. A total of 647 asymptomatic firefighters evaluated as a part of a wellness protocol were referred for cardiac multidetector computed tomography to evaluate abnormal exercise treadmill test findings. They were matched by age and cardiovascular risk factors, with 2,533 asymptomatic subjects undergoing cardiac computed tomography because of abnormal electrocardiographic or exercise treadmill test findings. CAC and the prevalence of obstructive coronary artery disease by vessel were derived. Finally, the predictors of CAC were analyzed using regression analysis. Of the firefighters, 49% had detectable CAC compared to 43% of controls (p = 0.015). Although the lesions were most prevalent in the left anterior descending artery in both groups, more firefighters had any left anterior descending artery stenosis compared to the controls (p <0.0001). The firefighters also had more left main coronary artery lesions than did the controls (p <0.0001). The firefighters had significantly greater CAC scores than did with the controls (p <0.001). Furthermore, the firefighters had significantly greater mean CAC scores (66 ± 8 in firefighters vs 33 ± 4 for controls, p <0.001). Firefighter status was independently associated with a 41-point increase in the CAC score (p <0.001). In conclusion, asymptomatic firefighters had more atherosclerosis and CAC than the matched controls.
Gated cardiac imaging, using 64-slice multidetector computed tomography (MDCT), has begun to gain acceptance as a coronary artery disease (CAD) risk stratification tool among asymptomatic patients. The County of Los Angeles Fire Department has initiated a comprehensive protocol designed, in part, to detect asymptomatic CAD. Prospective firefighters undergo a maximal effort treadmill exercise stress test before training. Employed firefighters undergo an annual medical examination, including a treadmill test as a “fitness for duty” examination. Cardiology follow-up is arranged for abnormal or equivocal treadmill test findings. Participation is encouraged although not mandatory. We hypothesized that firefighters would have more CAD, as determined by cardiac MDCT, than the general population, even after adjustment for conventional risk factors.
Methods
A total of 647 asymptomatic firefighters with abnormal treadmill test findings were referred for follow-up evaluation at a single facility (St. John’s Cardiovascular Research Center, Harbor-UCLA Medical Center, Torrance, California). All 647 firefighters underwent coronary artery calcium (CAC) and MDCT evaluation. This population has been previously described, although the present study included more subjects. The control sample was obtained from 2,533 asymptomatic subjects referred by their primary physician for CAC and MDCT after abnormal electrocardiographic or exercise treadmill test findings. The CAC scans were largely (78%) performed the same day as the exercise treadmill test, and 99% were done within 1 week. A stress test was considered abnormal (demonstrative of ischemia) in the presence of a 1-mm flat or downsloping ST depression, lasting 0.08 seconds for 3 consecutive beats.
All subjects were given a risk factor questionnaire to determine the ethnicity and presence of CAD risk factors according to the National Cholesterol Education Program guidelines. The risk factors included current cigarette smoking, diabetes, a history of premature CAD in a first-degree relative (men <45 years and women <55 years), hyperlipidemia, and hypertension. Hypertension was defined by the current use of antihypertension medicine or known, but untreated, hypertension. Current cigarette smoking was defined as cigarette use within the past month. Hyperlipidemia was defined as the current use of lipid-lowering agents or diagnosed, but untreated, hyperlipidemia (total serum cholesterol >200 mg/dl).
A risk factor composite score was computed for each subject, and the firefighters were subsequently matched with controls in a 1:4 fashion. The Institutional Review Board of Harbor-UCLA Medical Center approved the study.
All subjects underwent MDCT using a 64-slice computed tomography scanner (LightSpeed VCT 64-slice scanner, GE Medical Systems, Milwaukee, Wisconsin). CAC scans were performed using 3-mm contiguous scans from the carina to the apex of the heart, with electrocardiographic triggering of 60% to 70% of the RR interval. The CAC score was measured using 2.5-mm-thick slices. The subjects then had an intravenous catheter inserted in the antecubetal vein and underwent coronary computed tomographic angiography. To avoid the motion artifacts caused by an elevated heart rate, the subjects received intravenous doses of metoprolol (in 5-mg doses) as needed for a heart rate >60 beats/min. Nitroglycerin spray (0.4 μg) was administered just before the test. The patients received an intravenous infusion of 60 to 80 mg contrast (Visipaque [iodixanol] or Omnipaque [iohexol], GE Healthcare) timed to achieve aortic opacification. Coronary angiography was obtained during a short breath-hold. Detector collimation was set at 64 channels, with 0.625-mm per slice, gantry rotation speed at 350 ms per rotation, and tube voltage of 120 kV at a current of 335 to 770 mA during 55% of the cardiac cycle (diastole) and a reduction of the current by 50% during the remaining time of the RR interval. This technology allowed a reconstructed slice thickness of approximately 0.35 mm.
Continuous data are expressed as the mean ± SE and frequency data as proportions. Continuous variables and categorical variables were compared using analysis of variance and the chi-square statistic, respectively. Student’s t test was used to test differences in the characteristics between the firefighter and control cohorts. In all statistical analyses, 2-sided p values of < .05 were considered to indicate statistical significance. Multiple logistic regression models were used to evaluate the association of firefighting status, as well as traditional CAD risk factors, with CAC. The vessel lesions’ distribution was compared using the Kruskal-Wallis test. The following risk factors were included in the analysis: age, male gender, hyperlipidemia, current smoking, hypertension, diabetes, and firefighter occupation. All statistical analyses were performed using Stata software, version 10 (StataCorp, College Station, Texas) and SAS, version 9.1.3 (SAS Institute, Cary, North Carolina).
Results
A total of 647 firefighters (average age 47 ± 8 years, and 96% were men; Table 1 ) were included. Approximately 35% had a positive family history, 30% had hyperlipidemia, and 13% had hypertension. Of the 647 firefighters, 2% were currently smoking at the time of the study and 3% had diabetes. The control sample of 2,533 subjects was aged 49 ± 9 years, on average, and 91% were men. Of the controls, 36% had a positive family history, 44% had hyperlipidemia, and 19% had hypertension; 3% were smoking currently and 2% had diabetes mellitus.
| Variable | Firefighter (n = 647) | Control (n = 2,533) | p Value |
|---|---|---|---|
| Age (years) | 47 ± 8 | 49 ± 9 | <0.001 |
| Men | 96% | 91% | <0.001 |
| Family history | 35% | 36% | 0.6 |
| Current smoker | 2% | 3% | 0.44 |
| Diabetes mellitus | 3% | 2% | 0.92 |
| Hyperlipidemia ⁎ | 30% | 44% | <0.001 |
| Hypertension † | 13% | 19% | 0.01 |
⁎ Hyperlipidemia defined as current use of lipid-lowering agents or diagnosed, but untreated, hyperlipidemia (total serum cholesterol >200 mg/dl).
† Hypertension defined by current use of antihypertension medicine or known, but untreated, hypertension.
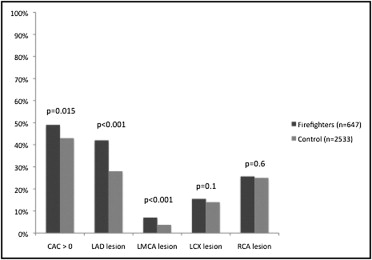
Approximately ½ (49%) of the firefighters had detectable CAC (score >0) compared to the controls (43%, p = 0.015; Figure 1 ) . Lesions were most commonly found in the left anterior descending artery (LAD) for both groups. Of the firefighters, 42% had any LAD lesion compared to 28% of the controls (p <0.0001). Lesions were rare in the left main artery for both groups. However, a statistically significant increase was found in firefighters with left main artery lesions compared to controls (7% vs 3.7%, p <0.0001). No significant differences were found between the left circumflex artery and right coronary artery lesions.
Firefighters had an average of 1.2 lesions in the LAD compared to controls, who had 0.7 lesions (p <0.0001). Although the prevalence of left main artery lesions was low, firefighters on average had more lesions in this vessel than controls (0.1 compared to 0.05, p = 0.03). No significant differences were seen in the number of lesions within the right coronary or circumflex arteries.
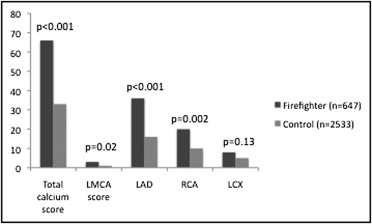
The total CAC was elevated among the firefighters ( Figure 2 ) . The mean CAC score for the firefighters was 66 ± 8 compared to 33 ± 4 for controls (p <0.001). CAC for both groups was predominantly found within the LAD artery, with firefighters having more calcium than controls (36 ± 4 compared to 16 ± 2, p <0.001). Firefighters also had higher CAC scores within the left main artery (3 ± 0.7) than controls (1 ± 0.2, p = 0.02) and in the right coronary artery (20 ± 3 in firefighters and 10 ± 1 in controls, p = 0.002). No statistically significant difference was seen for the left circumflex artery CAC score.