Aortic root dilation is important in the diagnosis of familial aortic syndromes, such as Marfan syndrome, and an important risk factor for aortic complications, such as dissection or rupture. Transthoracic echocardiography reliably measures the absolute aortic root size; however, the degree of abnormality of the measurement requires correction for the expected normal aortic root size for each patient. The expected normal size is currently predicted according to the body surface area (BSA) and age. However, the correlation between root size and BSA is imperfect, particularly for older patients. A potential exists to improve the diagnosis and treatment of patients with aortic disease, with an improved estimation of normal aortic root size. A reference size derived from within the cardiovascular system has been hypothesized to provide a more direct correlation with the aortic root size. Images from the Stanford echocardiography database were reviewed, and measurements of the aortic root and internal dimensions were performed in a control cohort (n = 150). The measurements were repeated in adult patients with Marfan syndrome (n = 70) on serial echocardiograms (145 total studies reviewed). Of the 150 control patients, excellent correlation was found between the aortic root and left ventricular outflow tract diameters, r 2 = 0.67, and r 2 = 0.34 with BSA (p <0.0001, for both). More importantly, using the left ventricular outflow tract to predict the normal aortic root size, instead of the BSA and age, improved the diagnostic accuracy of aortic root measurements for diagnosing Marfan syndrome. In conclusion, an internal cardiovascular reference, the left ventricular outflow tract diameter, can improve the diagnosis of aortic disease and might provide a better reference for the degree of abnormality.
Multiple studies have demonstrated that body size is a factor in determining the “normal” cardiovascular dimensions. As such, scaling to body size and age is frequently used in clinical practice to predict the normal aortic root dimensions. However, in patients >40 years old, the correlation of the aortic root diameter with the body surface area (BSA) is weak (r 2 = 0.16). We hypothesized that scaling the aortic root size to other cardiovascular dimensions might be more direct than scaling to the BSA and thus might be more precise. Our goals were fourfold: (1) to identify the cardiovascular dimensions that correlated tightly with aortic root size in those without aortic disease; (2) to demonstrate that these dimensions have a narrower distribution of normal values and, thus, more accurately predict the normal aortic size and identify aortic root disease; and (3) to determine whether the diagnosis of abnormal aortic root size using such dimensions is superior to the BSA in patients with a diagnosis of Marfan syndrome. Finally, (4) to make the selected reference cardiovascular measurement useful, we needed to also demonstrate that it is not affected by the disease process leading to aortic root enlargement.
Methods
Two-dimensional transthoracic echocardiographic images from the adult Stanford echocardiography database were reviewed. The Stanford University institutional review board approved the present study (protocol 19172). A representative control cohort of 150 subjects was chosen from the Stanford Cardiovascular Aging Study and the echocardiography database. Controls were selected in reverse chronologic fashion from the databases to include the desired number from each of several age ranges and both genders. The controls included normal subjects (all dimensions, including ejection fraction and valvular parameters, were within normal limits within the European Association of Echocardiography/American Society of Echocardiography guidelines) and subjects with a variety of cardiac conditions. We included patients with severe heart failure and severe valvular disease (excluding only aortic regurgitation) to represent the population in whom we wanted to identify aortic abnormalities. Excluded were only those with conditions in which the aortic and left ventricular outflow tract (LVOT) diameter would not be expected to be normal (i.e., a history of aortic root or aortic valve repair/replacement, malformed and bicuspid aortic valves, cardiac transplantation, more than mild aortic regurgitation, hypertrophic cardiomyopathy), patients <18 years old, and those with poor image quality.
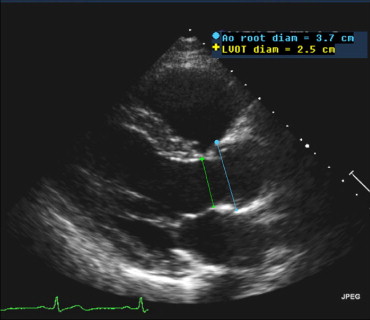
The internal cardiac dimensions, including aortic root diameter, LVOT diameter, and left ventricular and atrial dimensions were measured. The aortic root and LVOT diameters were measured on parasternal long-axis views at their maximum dimension, typically at end-systole ( Figure 1 ). The aortic root diameter was measured using the leading edge to leading edge technique. The LVOT was measured at the level of the aortic annulus using a standard black–white interface measurement. The height and weight were known for all patients, and the BSA was calculated using DuBois and DuBois.
The measurements were made on serial echocardiograms from a cohort of patients with Marfan syndrome (n = 70, 145 total studies reviewed) to prove validity in the population of interest. The patients were taken at random from the adult Marfan clinic roster, were >18 years old, and had not undergone aortic root surgery. All had been diagnosed with Marfan syndrome by the 1996 Ghent diagnostic criteria, which include the aortic criteria dependent on the BSA. Excluded were patients with greater than mild aortic regurgitation, but patients with significant mitral regurgitation were included.
The relation between continuous variables was tested using linear regression models. The 95% confidence intervals were calculated, and analysis of variance was performed. The receiver operating characteristic curves and area under the curve were computed. Analysis was done using JMP, version 7, software (SAS Institute, Cary, North Carolina) and MedCalc software (Mariakerke, Belgium), with a significance level of p = 0.05.
Results
The patient characteristics are listed in Table 1 . The control patients were significantly older and shorter than those with Marfan syndrome. Inherent to the diagnosis of Marfan syndrome, and therefore expected, those with Marfan syndrome had larger aortic root diameters. Although the patients with Marfan syndrome also had larger LVOT sizes, the range did not significantly exceed the range in the controls.
| Patient Group | Control Group (n = 150) | Marfan Group (n = 70) | p Value |
|---|---|---|---|
| Men (n) | 71 (47%) | 34 (49%) | — |
| Age (years) | <0.0001 | ||
| Mean ± SD | 49 ± 18 | 33 ± 12 | |
| Median | 46 | 31 | |
| Range | 22–90 | 18–64 | |
| Height (cm) | <0.0001 | ||
| Mean ± SD | 169 ± 10 | 185 ± 10 | |
| Median | 168 | 186 | |
| Range | 130–193 | 167–210 | |
| Weight (kg) | 0.009 | ||
| Mean ± SD | 74 ± 23 | 83 ± 24 | |
| Median | 69 | 76 | |
| Range | 43–182 | 45–168 | |
| Body surface area (m 2 ) | <0.0001 | ||
| Mean ± SD | 1.83 ± 0.27 | 2.05 ± 0.28 | |
| Median | 1.80 | 2.00 | |
| Range | 1.34–2.92 | 1.50–2.73 | |
| Aortic root diameter (cm) | <0.0001 | ||
| Mean ± SD | 3.26 ± 0.31 | 4.42 ± 0.52 | |
| Median | 3.30 | 4.40 | |
| Range | 2.60–4.00 | 3.5–5.9 | |
| Left ventricular outflow tract diameter (cm) | <0.0001 | ||
| Mean ± SD | 2.15 ± 0.24 | 2.42 ± 0.21 | |
| Median | 2.10 | 2.40 | |
| Range | 1.70–2.80 | 2.00–2.90 |
The aortic root diameter correlated with multiple internal cardiac dimensions measured in the control cohort. The correlation (r 2 ) of the LVOT diameter was identified as the strongest correlation (r 2 = 0.67), although the correlation with BSA was only 0.34 (p <0.0001 for all; Table 2 ).
| Group | LVOT | Height | Weight | BSA | BMI | Age |
|---|---|---|---|---|---|---|
| All controls (n = 150) | 0.67 | 0.30 | 0.24 | 0.34 | 0.10 | 0.00 |
| Age <40 years (n = 47) | 0.62 | 0.28 | 0.23 | 0.32 | 0.13 | 0.01 |
| Age >40 years (n = 103) | 0.69 | 0.35 | 0.25 | 0.35 | 0.09 | 0.00 |
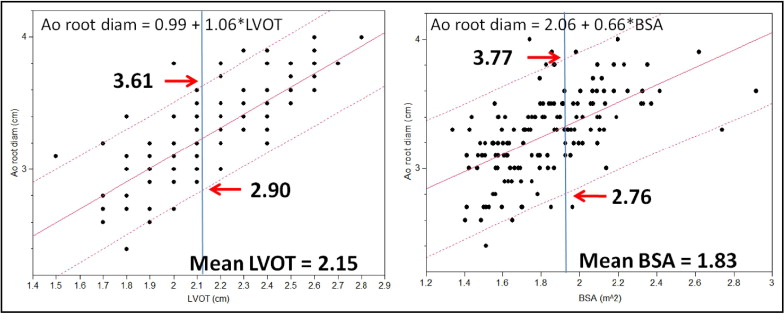
The aortic root size when plotted against the LVOT showed a line of best fit with a slope of 1.06. In contrast, the slope was 0.66 when the aortic root size was plotted against the BSA. The bivariate fit models and 95% confidence intervals are shown in Figure 2 . The clinical value of the improved correlation is also shown in Figure 2 , where, at the mean LVOT of 2.15 cm, the range of the normal aortic dimension is 2.90 to 3.61 cm, and at a mean BSA of 1.83 cm, it is 2.76 to 3.77 cm. Using LVOT for normalization, the prediction of the normal aortic size is more precise by 3 mm.