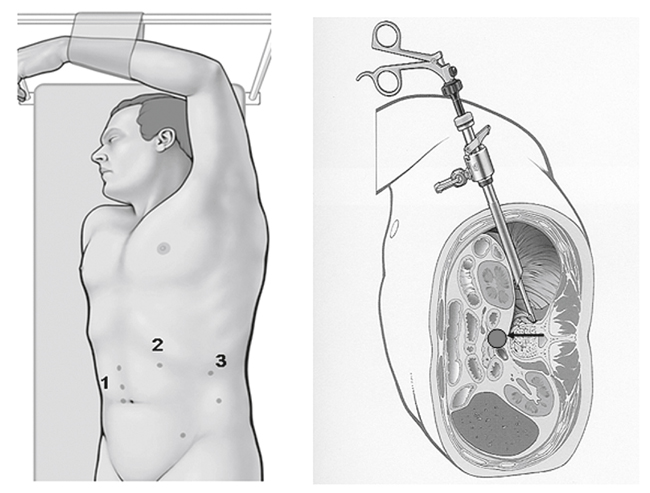
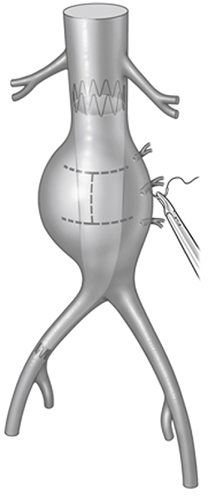
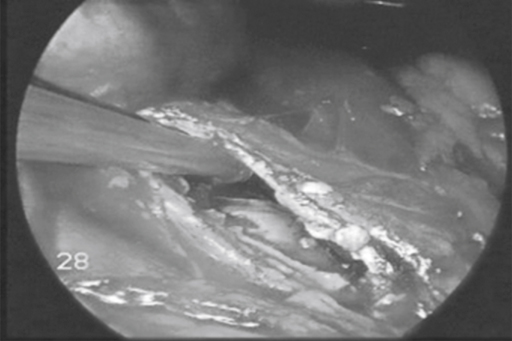
A pneumoperitoneum is established and the abdomen is inspected. A transperitoneal retrocolic access combined with medial mobilization of the left kidney is preferred (Figure 1). Alternatively, the left kidney can be left in situ. For more complex total laparoscopic operations like conversion after EVAR, up to eight trocars are required. The sac of the aneurysm is incised and opened with laparoscopic scissors in an H-shaped configuration (Figure 2). The graft is inspected using the magnification of the 30-degree endoscope to exclude any damage of the fabric or stents. Laparoscopic graspers and a 10-mm suction–irrigation device are used to remove the thrombus material. Patent lumbar arteries are stitched from within using Vicryl sutures. The surgeon is standing on the right side of the patient. In addition to these steps, bioglues can be injected into the sac of the aneurysm to accelerate graft incorporation and to prevent any backbleeding from the lumbar arteries (Figure 3). With a laparoscopic running suture (2–0 Prolene), the sac of the aneurysm is closed, wrapping the aorta tightly around the endograft.
Combined Laparoscopic and Endovascular Treatment of Aortic Diseases
Operative Technique
Laparoscopic Remodelling of the Aorta After Endovascular Aneurysm Repair
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


