Coagulopathy and Thrombophilia This is broadly explained with Virchow’s Triad: Stasis of blood flow, Injury (tissue factor exposure) and Hypercoagulopathy. A hypercoagulopathy is an inherent and intrinsic increased tendency towards thrombosis. It affects both venous (most common) and arterial systems and is classified as either primary or secondary. Coagulation and haematology including prothrombin time, APTT, international normalised ratio (INR), FBC (platelets), platelet aggregation, tests for malignancy (if indicated). D-dimer assay. D-dimers are breakdown products of cross-linked fibrin and represent a very sensitive marker of thrombosis–fibrinolysis with a high negative predictive value. Therefore a normal test (in conjunction with a negative U/S if indicated) effectively excludes a venous thrombotic event with very high certainty. However, it is also very non-specific, rising in many other disease states (e.g. post-operative, malignancy, sepsis). Thrombophilia screen. This is a test for primary hypercoagulopathy when an inherited or familial thrombophilia is suspected. It is useful to consult with a haematologist because not all patients require testing, but in general the following groups of patients warrant screening: young (<40 years), familial history, recurrent thrombosis (with no identifiable cause) and ‘unusual’ venous thrombosis (e.g. mesenteric, cerebral).
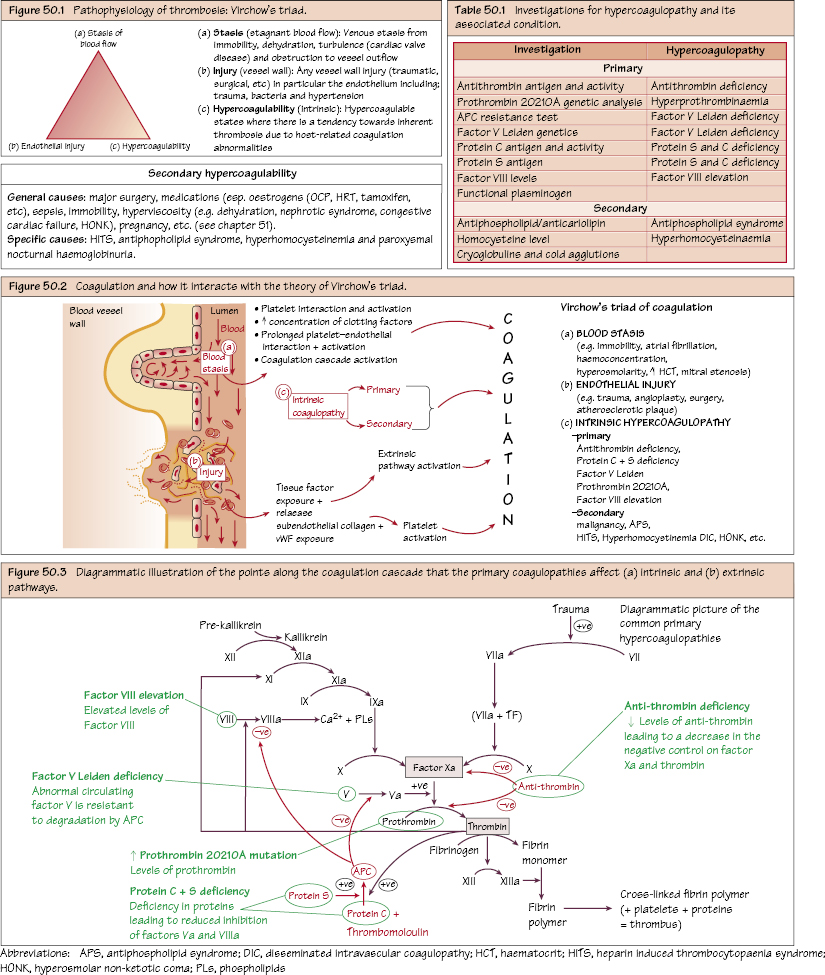
Pathophysiology of Thrombosis
Hypercogulopathy
Investigations
Primary Hypercoagulability
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


